Download
1 / 1
10 likes | 72 Views
The study evaluates the effectiveness of "The Airway Programme" (TAP) in improving outcomes for patients with COPD in Singapore. Participating in TAP was associated with lower mortality rates but higher risk of readmission. Further research is needed to adjust for biases and assess causality.

E N D
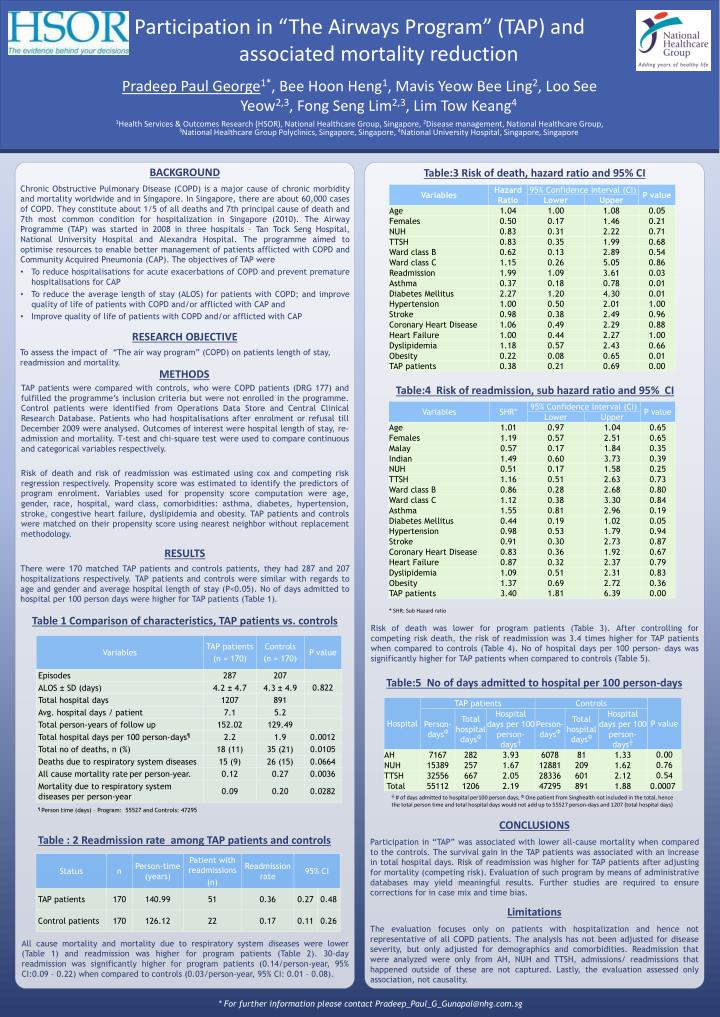
Table:3 Risk of death, hazard ratio and 95% CI Chronic Obstructive Pulmonary Disease (COPD) is a major cause of chronic morbidity and mortality worldwide and in Singapore. In Singapore, there are about 60,000 cases of COPD. They constitute about 1/5 of all deaths and 7th principal cause of death and 7th most common condition for hospitalization in Singapore (2010). The Airway Programme (TAP) was started in 2008 in three hospitals – Tan Tock Seng Hospital, National University Hospital and Alexandra Hospital. The programme aimed to optimise resources to enable better management of patients afflicted with COPD and Community Acquired Pneumonia (CAP). The objectives of TAP were To reduce hospitalisations for acute exacerbations of COPD and prevent premature hospitalisations for CAP To reduce the average length of stay (ALOS) for patients with COPD; and improve quality of life of patients with COPD and/or afflicted with CAP and Improve quality of life of patients with COPD and/or afflicted with CAP BACKGROUND RESEARCH OBJECTIVE CONCLUSIONS Participation in “TAP” was associated with lower all-cause mortality when compared to the controls. The survival gain in the TAP patients was associated with an increase in total hospital days. Risk of readmission was higher for TAP patients after adjusting for mortality (competing risk). Evaluation of such program by means of administrative databases may yield meaningful results. Further studies are required to ensure corrections for in case mix and time bias. Limitations The evaluation focuses only on patients with hospitalization and hence not representative of all COPD patients. The analysis has not been adjusted for disease severity, but only adjusted for demographics and comorbidities. Readmission that were analyzed were only from AH, NUH and TTSH, admissions/ readmissions that happened outside of these are not captured. Lastly, the evaluation assessed only association, not causality. To assess the impact of “The air way program” (COPD) on patients length of stay, readmission and mortality. 1Health Services & Outcomes Research (HSOR), National Healthcare Group, Singapore, 2Disease management, National Healthcare Group, 3National Healthcare Group Polyclinics, Singapore, Singapore, 4National University Hospital, Singapore, Singapore Pradeep Paul George1*, Bee Hoon Heng1, Mavis Yeow Bee Ling2, Loo See Yeow2,3, Fong Seng Lim2,3, Lim Tow Keang4 Participation in “The Airways Program” (TAP) and associated mortality reduction METHODS TAP patients were compared with controls, who were COPD patients (DRG 177) and fulfilled the programme’s inclusion criteria but were not enrolled in the programme. Control patients were identified from Operations Data Store and Central Clinical Research Database. Patients who had hospitalisations after enrolment or refusal till December 2009 were analysed. Outcomes of interest were hospital length of stay, re-admission and mortality. T-test and chi-square test were used to compare continuous and categorical variables respectively. Risk of death and risk of readmission was estimated using cox and competing risk regression respectively. Propensity score was estimated to identify the predictors of program enrolment. Variables used for propensity score computation were age, gender, race, hospital, ward class, comorbidities: asthma, diabetes, hypertension, stroke, congestive heart failure, dyslipidemia and obesity. TAP patients and controls were matched on their propensity score using nearest neighbor without replacement methodology. Table:4 Risk of readmission, sub hazard ratio and 95% CI RESULTS There were 170 matched TAP patients and controls patients, they had 287 and 207 hospitalizations respectively. TAP patients and controls were similar with regards to age and gender and average hospital length of stay (P<0.05). No of days admitted to hospital per 100 person days were higher for TAP patients (Table 1). * SHR: Sub Hazard ratio Table 1 Comparison of characteristics, TAP patients vs. controls Risk of death was lower for program patients (Table 3). After controlling for competing risk death, the risk of readmission was 3.4 times higher for TAP patients when compared to controls (Table 4). No of hospital days per 100 person- days was significantly higher for TAP patients when compared to controls (Table 5). Table:5 No of days admitted to hospital per 100 person-days ┼ # of days admitted to hospital per100 person days, ΦOne patient from Singhealth not included in the total, hence the total person time and total hospital days would not add up to 55527 person-days and 1207 (total hospital days) ¶ Person time (days) – Program: 55527 and Controls: 47295 Table : 2 Readmission rate among TAP patients and controls All cause mortality and mortality due to respiratory system diseases were lower (Table 1) and readmission was higher for program patients (Table 2). 30-day readmission was significantly higher for program patients (0.14/person-year, 95% CI:0.09 – 0.22) when compared to controls (0.03/person-year, 95% CI: 0.01 – 0.08). * For further information please contact Pradeep_Paul_G_Gunapal@nhg.com.sg






















