Download
1 / 54
640 likes | 1.2k Views
Adrenergic Antagonists. These drugs act by either reversibly or irreversibly attaching to the receptor, thus preventing its activation by endogenous catecholamines .

E N D
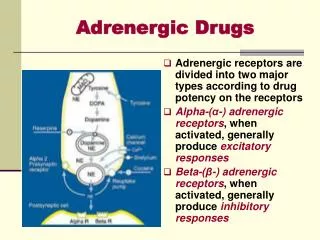
These drugs act by either reversibly or irreversibly attaching to the receptor, thus preventing its activation by endogenous catecholamines. • Adrenergic antagonists are classified according to their relative affinities for α or β receptors in the peripheral nervous system.
α-ADRENERGIC BLOCKING AGENTS • α adrenoceptors blockers profoundly affect blood pressure. • Decrease in TPR • This induces a reflex tachycardia. • Effects are more profound in an individual who is standing and less in a person who is supine.
A. Phenoxybenzamine • Nonselective: α1- and α2-receptors. • Blocks acetylcholine, histamine, and serotonin receptors • The block is irreversible and noncompetitive. • Long-acting: last about 24 hours after a single administration.
1. Actions: Cardiovascular effects: • Alpha 1 action: • It prevents vasoconstriction of peripheral blood vessels • The decreased peripheral resistance provokes a reflex tachycardia. • Presynaptic α2 receptors in the heart: • increases cardiac output. • Unsuccessful in maintaining lowered blood pressure in hypertension, and its use has been discontinued for this purpose.
2. Therapeutic uses Phenoxybenzamine: • Treatment of pheochromocytoma. • Phenoxybenzamine is sometimes effective in treating Raynaud disease, frostbite, and acrocyanosis. • Management of autonomic hyperreflexia.
3. Adverse effects of Phenoxybenzamine: • Postural hypotension • nasal stuffiness • Nausea • Vomiting • It may inhibit ejaculation. • It may induce reflex tachycardia.
B. Phentolamine • Competitive blocker of α1 and α2 receptors. • Duration of action: approximately 4 hours • Potent vasodilator, but induces pronounced reflex tachycardia • blocking the α2 receptors of the cardiac sympathetic nerves causes cardiac stimulation
Phentolamine is used for: • the short-term management of pheochromocytoma. • used locally to prevent dermal necrosis and extravasation due to norepinephrine administration • used to treat hypertensive crisis due to: • abrupt withdrawal of clonidine • from ingesting tyramine-containing foods in patients taking nonselective monoamine oxidase inhibitors.
C. Selective competitive blockers of the α1 receptor PrazosinTerazosinDoxazosinTamsulosinAlfuzosin • Prazosin, terazosin, doxazosin: treatment of hypertension. • Tamsulosin and alfuzosin: treatment of benign prostatic hypertrophy (BPH). • Doxazosin is the longest acting of these drugs.
1. Cardiovascular effects: • They decrease peripheral vascular resistance and lower arterial blood pressure by causing the relaxation of both arterial and venous smooth muscle. • They cause minimal changes in: • cardiac output • renal blood flow • glomerular filtration rate.
2. Therapeutic uses: • Treatment of hypertension • The first dose of these drugs produces an exaggerated orthostatic hypotensive response that can result in syncope (fainting). • This action, termed a “first-dose” effect, may be minimized by: • adjusting the first dose to one-third or one-fourth of the normal dose • giving the drug at bedtime. • These drugs improve lipid profiles and glucose metabolism in hypertensive patients.
Prazosin and others are used to treat congestive heart failure. • By dilating both arteries and veins, these agents decrease preload and afterload, leading to an increase in cardiac output and a reduction in pulmonary congestion. • Tamsulosinis an inhibitor (with some selectivity) of the α1A receptors found on the smooth muscle of the prostate.
3. Adverse effects: • Dizziness • A lack of energy • nasal congestion • Headache • Drowsiness • orthostatic hypotension. • Prazosin Should be given along with a diuretic : retain sodium (Na+) and fluid.
Tamsulosin has a caution about “floppy iris syndrome,” a condition in which the iris swells out in response to intraoperative eye surgery.
D. Yohimbine Selective competitive α2 blocker • It is found as a component of the bark of the yohimbe • Sometimes used as a sexual stimulant. • Yohimbine works at the level of the CNS to increase sympathetic outflow to the periphery.
III. β-ADRENERGIC BLOCKING AGENTS • Competitive antagonists. • Non-selective:β1 and β2 receptors • Cardioselectiveβ antagonists primarily block β1 receptors • β blockers are effective in treating • Angina • cardiac arrhythmias • myocardial infarction • congestive heart failure • Hyperthyroidism • Glaucoma • prophylaxis of migraine headaches. The names of all β blockers end in “-olol” except for labetalol and carvedilol.
A. Propranolol: prototype β-adrenergic antagonist • A nonselective β antagonist: blocks both β1 and β2 receptors with equal affinity • Sustained-release preparations for once-a-day dosing are available. 1. Actions: • Cardiovascular: • Diminishes cardiac output: • having negative inotropic and chronotropic effects . • It directly depresses sinoatrial and atrioventricular activity.
b. Peripheral vasoconstriction: • Blockade of β receptors prevents β2-mediated vasodilation. CO BP reflex peripheral vasoconstriction. • No postural hypotension occurs, because the α1-adrenergic receptors that control vascular resistance are unaffected.
Bronchoconstriction: • This can precipitate a respiratory crisis in patients with chronic obstructive pulmonary disease (COPD) or asthma. d. Increased Na+ retention: • Reduced blood pressure causes a decrease in renal perfusion, resulting in an increase in Na+ retention and plasma volume. • In some cases, this compensatory response tends to elevate the blood pressure. For these patients, β blockers are often combined with a diuretic to prevent Na+ retention
e. Disturbances in glucose metabolism: • β Blockade leads to decreased: • Glycogenolysis • glucagon secretion. • Therefore, if a patient with type 1 diabetes is to be given propranolol, very careful monitoring of blood glucose is essential, because pronounced hypoglycemia may occur after insulin injection. • β Blockers also attenuate the normal physiologic response to hypoglycemia.
Because of its ability to suppress glycogenolysis and mask tachycardia, propranolol must be used with caution by diabetic patients."
2. Pharmacokinetics: • After oral administration, propranolol is almost completely absorbed. • It is subject to first-pass effect, and only about 25 percent of an administered dose reaches the circulation. • it is highly lipophilic and readily crosses the blood-brain barrier. • Propranolol is extensively metabolized, and most metabolites are excreted in the urine.
3. Therapeutic effects: a. Hypertension: • by several different mechanisms of action. • Decreased cardiac output is the primary mechanism • inhibition of renin release from the kidney • decrease in total peripheral resistance with long term use • decreased sympathetic outflow from the CNS
b. Migraine: • Propranolol is also effective in reducing migraine episodes when used prophylactically. • β Blockers decrease the incidence and severity of the attacks. c. Hyperthyroidism: • Propranolol and other β blockers are effective in blunting the widespread sympathetic stimulation that occurs in hyperthyroidism. • In acute hyperthyroidism (thyroid storm), β blockers may be lifesaving in protecting against serious cardiac arrhythmias.
d. Angina pectoris: • Propranolol decreases the oxygen requirement of heart muscle and, therefore, is effective in reducing the chest pain on exertion that is common in angina. • Propranolol is, thus, useful in the chronic management of stable angina but not for acute treatment.
e. Myocardial infarction: • Administration of a β blocker immediately following a myocardial infarction reduces infarct size and hastens recovery. • Used prophylactically after an MI. • Protective effect on the myocardium: blocking of the actions of circulating catecholamines, which would increase the oxygen demand in an already ischemic heart muscle. • Propranolol also reduces the incidence of sudden arrhythmic death after myocardial infarction.
4. Adverse effects: The reasons for this are not clear and may be independent of β-receptor blockade. • The β blockers must be tapered of gradually for at least a few weeks.
Metabolic disturbances: • β Blockade: decreases glycogenolysis and glucagon secretion. • Fasting hypoglycemia may occur. • In addition, β blockers can prevent the counter regulatory effects of catecholamines during hypoglycemia. • The perception of symptoms such as tremor, tachycardia, and nervousness are blunted. • Patients administered nonselective β blockers have: • increased low-density lipoprotein • increased triglycerides • reduced high-density lipoprotein
e. CNS effects: • Propranolol has numerous CNS-mediated effects, including: • Depression • Dizziness • Lethargy • Fatigue • Weakness • visual disturbances • Hallucinations • short-term memory loss • emotional liability • vivid dreams (including nightmares) • decreased performance • insomnia.
f. Drug interactions: • Drugs that interfere with, or inhibit, the metabolism of propranolol, such as cimetidine, fluoxetine, paroxetine, and ritonavir, may potentiate its antihypertensive effects. • Conversely, those that stimulate or induce its metabolism, such as barbiturates, phenytoin, and rifampin, can decrease its effects.
B. Timolol and nadolol: Nonselective β antagonists • More potent than propranolol. • Nadolol has a very long duration of action. • Timolol reduces the production of aqueous humor in the eye. • It is used topically in the treatment of chronic open-angle glaucoma.
1. Treatment of glaucoma: • Topically applied agents: timolol, betaxolol, or carteolol • They decrease the secretion of aqueous humor by the ciliary body. • Chronic use : The β blockers • Acute attack of glaucoma: pilocarpine is the drug of choice. • Onset: 30 minutes • Duration of action: 12 to 24 hours.
C. Selective β1 antagonists: • Acebutolol • Atenolol • Metoprolol • Bisoprolol • Betaxolol • Nebivolol • Esmolol • This cardio selectivity is: • most pronounced at low doses • lost at high doses
Actions: • These drugs: • lower blood pressure in hypertension • increase exercise tolerance in angina. • Esmolol has a very short lifetime ( 10 min.) due to metabolism of an ester linkage. • Nebivololalso has vasodilator properties mediated by nitric oxide.
2. Therapeutic use in hypertension: • The cardioselective β blockers are useful in hypertensive patients with impaired pulmonary function. • Because these drugs have less effect on peripheral vascular β2 receptors. • Cardioselective β blockers are useful in diabetic hypertensive patients.
D. Antagonists with partial agonist activity: Pindolol and acebutolol 1. Actions: • Cardiovascular: • They are not pure antagonists, they are partial agonists. • They have intrinsic sympathomimetic activity (ISA). • Decreased metabolic effects: • Minimal effect on lipid and carbohydrate metabolism. • For example, these agents do not decrease plasma HDL levels.
2. Therapeutic use in hypertension: • Hypertensive patients with moderate bradycardia: because a further decrease in heart rate is less pronounced with these drugs. • Diabetic hypertensive patients: carbohydrate metabolism is less affected.
E. Antagonists of both α and β adrenoceptors:Labetalol and carvedilol 1. Actions: • α1-blocking actions: produce peripheral vasodilation, thereby reducing blood pressure. • They do not alter serum lipid or blood glucose levels. • Carvedilol also decreases lipid peroxidation and vascular wall thickening, effects that have benefit in heart failure. 2. Therapeutic use in: • hypertension • heart failure
Labetalolmay be used as: • an alternative to methyldopa in the treatment of pregnancy-induced hypertension. • Intravenously to treat hypertensive emergencies, because it can rapidly lower blood pressure. • Carvedilol: • Clinical trials have shown that carvedilol has clinical benefits in patients with stable chronic heart failure. • It can reduce mortality and hospitalization in this population.
3. Adverse effects: associated with α1 blockade • Orthostatic hypotension • Dizziness.