Download
1 / 61
640 likes | 997 Views
Basic Principles and Difficult Pain. Dr Pete Nightingale Macmillan GP. Objectives. By the end of this session I hope that you will have refreshed your ability to diagnose the type of pain a patient has and have in mind a strategy to deal with each pain. Incidence in Cancer.

E N D
Basic Principles and Difficult Pain Dr Pete Nightingale Macmillan GP
Objectives By the end of this session I hope that you will have refreshed your ability to diagnose the type of pain a patient has and have in mind a strategy to deal with each pain.
Incidence in Cancer • About ¼ of patients never have pain • Of those that do:- • 1/3 have a single pain • 1/3 have three or more different pains
Overview of Pain Classification • Definitions • Classification • Nociceptive and Neuropathic
Definitions of Pain • Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage • Allodynia Pain due to a stimulus that does not normally provoke pain • Dysaesthesia An unpleasant abnormal sensation, whether spontaneous or evoked
Causes of Pain • Pain caused by cancer and other medical illnesses may be caused by either direct effect of the disease OR • By the treatment associated with the disease which injure organs,muscles and nerves.E.G. Surgery, Chemo, XRT
Which type of pain could be classified as visceral nociceptive pain? • A Dull or aching, well localised • B Intermittant, burning or shooting • C Associated with an area of abnormal sensation • D Poorly localised, colic or sensation of pressure
Classification of Pain Nociceptive Pain Neuropathic Pain Pain pathways intact Anatomical or functional abnormality of pain pathway In area of abnormal sensation Somatic Visceral
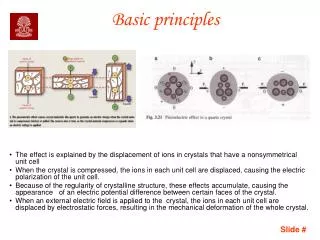
Nociceptive Pain • Somatic Activation of pain receptors (nociceptors) by chemical stimuli in cutaneous or deep tissues • Visceral Activation of nociceptors as a result of infiltration/compression/extension or stretching of viscera (organs)
Neurophysiology • Normal physiology of pain DRG CNS Pain neurone Stimulus Response
Normal Sensation Low intensity stimulation High Intensity Stimulation Innocuous Sensation PAIN
Neuropathic Pain • Spontaneous firing of damaged nerves • Pain due to a disturbance or pathological change in a nerve • A form of pain that occurs in up to 1% of population. • Virtually any condition that damages neural tissue or causes neuronal dysfunction can result in neuropathic pain • Pain in an area of abnormal sensation
Diagnosis SYMPTOMS SIGNS • Positive • Pain • Paraesthesia • Hyperaesthesia • Negative • Numbness • Normal • Motor • Distal Wasting • Absent reflexes • Sensory • Reduced Vibration/ light touch/ Pinprick
Assessment of Pain • History ‘ Pain is what the patient says it is’ There is evidence health workers tend to underestimate pain. PQRST Response to previous treatment New Pain or Exacerbation
P P Q R S T • P Palliative factors ‘what makes it better?’ • P Provocative factors ‘what makes it worse?’ • Q Quality of pain ‘what exactly is it like?’ • R Radiation ‘Does it spread anywhere?’ • S Severity ‘How much is it affecting life?’ • T Temporal factors ‘Does the pain come and go?’
Assessing Consequences of Pain PAIN MAY LEAD TO depression Anxiety Ability to interact socially physical performance working ability family income
Treating the Underlying Cause • Palliative Anti-cancer Treatment Radiotherapy Chemotherapy Hormone therapy • Modifying the effects of the disease Correct Hypercalcaemia Treat Lymphoedema Surgery – spinal stabilisation
WHO Analgesic LadderWill deal with 80% of Cancer Pain strong opioid (morphine) weak opioid (Codeine or Tramadol) non-opioid (Paracetamol) +/- Adjuvant
Tramadol • Dual MOA • Via opioid receptors • By blocking 5HT and NA • 1/5th as potent as morphine orally • Less constipating than codeine/morphine • ?role in neuropathic pain • ?lowers seizure threshold
Rules for Step 2 • A weak opioid should be added to a non-opioid • If a weak opioid is inadequate at regular optimal dose, change to morphine • Codeine is 1/10th as potent as morphine • Do not ‘kangaroo’ from weak opioid to weak opioid
Step3: Strong Opioids • Morphine • Diamorphine • Oxycodone • Methadone • Hydromorphone • Fentanyl • Alfentanil
Yet another A B C ! • A-Anti-emetic-usually Haloperidol 1.5mg for 7-10 days • B- Breakthrough pain. Use 1/6 of daily dose (4 hrly equivalent) as ‘rescue’ • C-Constipation – Laxative always required
Morphine preparations • Modified Release: Zomorph /MST Continus 12 hourly regularly MXL capsules 24 hourly regularly
Initiation of Morphine • For uncontrolled pain, start 4 hourly I/R morphine for rapid titration • Prescribe prn I/R at the same dose • If the patient responds to rescue doses, use them as needed • (? double night-time dose)
Conversion to long acting • Once pain controlled on 4 hourly dose I/R morphine, can convert to M/R morphine • Tot up total daily morphine • For Zomorph: divide by 2 and prescribe Zomorph at this dose bd • For MXL: prescribe the total dose once daily
Conversion • Prescribe prn breakthrough dose 1/6th of total daily morphine dose • Give the 1st dose of M/R morphine with the last regular dose of I/R
Patient Explanation • The first goal is reduction in discomfort (setting targets) • Common side-effects are sleepiness, nausea and constipation. • The drowsiness/nausea tend to wear off • Prophylactic Rx nausea and constipation THEN REGULARLY REVIEW PATIENT
Choosing the right opioid Subcutaneous infusion: diamorphine Stable pain, unable to swallow: SC diamorphine or transdermal fentanyl Afraid of using morphine: oxycodone or fentanyl Infection with pyrexia: any can be used except transdermal fentanyl Mild - moderate renal impairment: Possibly use hydromorphone Severe renal failure: fentanyl Liver impairment: morphine (with care)
Please rank the following in order of potency:- • A Codeine 60mg • B Tramadol 100mg • C Morphine 5mg • D Fentanyl 25mcg/hr patch.
FENTANYL (eg Durogesic D Trans) • Alternative strong opioid (Change patch every 72 hrs) • Take 12-48hrs to achieve maximum blood levels • Oral Morphine used for breakthrough pain • Indications for use • Intolerable adverse effects of morphine • Tablet phobia or difficulty swallowing • Poor compliance with oral medication • When the patient won’t have anything called morphine!
Oxycodone • MR – Oxycontin IR – Oxynorm • Oxycodone twice as potent as morphine • MST 10mg bd Oxycontin 5mg bd • Tolerated better by some • More expensive
Non-drug Treatments (1) • Nerve Blocks Local Anaesthetic Neurolytic (phenol) • Neurosurgery Cordotomy • Immobilisation Rest / Slings /Splints/ Corset Walking Aids / Wheelchair
Non-drug Treatments (2) • Psychology Individual Group Relaxation Education Cognitive Therapy Multi-disciplinary Approach • Distraction • Hypnosis
Mannix K et al Palliative Medicine 2006; 20:579-584 Cognitive Behaviour Therapy (CBT) can be used by palliative care staff to help patients. Training may become more widely available
CBTCognitive Behaviour Therapy Physical Pain
ABC of CBT! • A is the activating event • B is your beliefs and thoughts • C is the consequences, such as emotions you feel
The Mercedes Model Our ever present internal states consist of: THINKING EMOTIONS PHYSIOLOGY
Non-drug Treatments (3) • Counter-irritation Massage – Gate Control Theory TENS – Gate Control Theory Acupuncture – stimulates release of endorphins • Physical Exercise and mobility Physiotherapy Hydrotherapy Music/ Art therapy • Lifestyle Modification