Download
1 / 21
210 likes | 297 Views
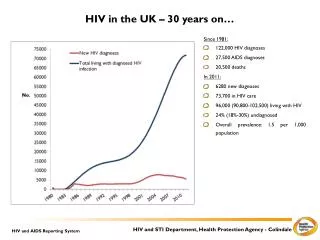
The UK Collaborative HIV Cohort (UK CHIC) Study. Background. Information on HIV infection in the UK comes from a variety of sources; these are often limited in scope Many clinical centres routinely collect information about HIV-positive patients when they attend:

E N D
Background • Information on HIV infection in the UK comes from a variety of sources; these are often limited in scope • Many clinical centres routinely collect information about HIV-positive patients when they attend: • This provides an ideal opportunity to study HIV-positive individuals in their clinical setting. • Existing infrastructure can be used for data collection. • Patients from a wide variety of clinics are included so that the cohort becomes more representative of HIV-positive people in the UK.
UK CHIC: Objectives • UK CHIC initiated in 2001 to collate routinely collected data from HIV-positive patients attending some of the largest clinical centres in the UK since 1st January 1996 • Specific aims are: • to describe the characteristics of patients with HIV under care • to provide information on exposure to combination antiretroviral therapy (cART) and changes to the immunological, virological and clinical status of patients over time • to monitor the frequency of AIDS and survival over time.
Inclusion criteria • Patients: • aged > 16 years and seen at any of the centres since 1/1/1996 • Clinics: • electronic data are already available • able to provide data on an annual basis
Funding • Study funded by the MRC since 2001 • Funding provides: • some database programming support • project co-ordination • statistical support • limited funding for clinics for provision of data • The database is physically located at MRC CTU – centrally located and ‘independent’ of all clinical centres • The project co-ordinator and principal investigator are based at UCL (Royal Free campus)
Study management Steering committee meets every 3-6 months with representatives from: • - each clinical centre • - the coordinating centre • - the UK Resistance Database • - the patient community Specific sub-groups: - data management - viral hepatitis co-infection - pregnancy - HIV and ageing - renal outcomes
Data protection policy • Policy drafted by a sub-group with input from experts in health informatics. • Data are submitted by secure web-based transfer (FTP), plus encryption. • Database access is restricted and monitored. • Datasets released for research analyses are approved by the steering committee, are anonymised, and only include necessary data. • Personnel with access to the data are made aware of data confidentiality requirements.
Processes Datasets and formats agreed upon by all centres Data sent to coordinator by centres Data checked for consistency Data entered into main database; error and logical checks performed Data from all centres merged and possible duplicates identified Final dataset distributed for analysis Errors checked and corrected on source and submitted dataset Results fed back to clinics and data managers Subset of records audited
Datasets HLA-B*5701 Hepatitis - A/B/C tests - clinical data Attendance Clinical events - AIDS - serious non-AIDS - death Demographics (patient, centre, ethnicity, risk group, first and last attendance) Antiretroviral therapy Adherence Prophylaxis (PCP) (No longer collected) CD4 viral loads Laboratory-defined toxicities ? future data items
Data quality checks • missing data items (demographics, drug names, CD4/CD8 counts, HIV RNA) • duplicate patients within same centre • duplicate laboratory measurements or AIDS events • undetectable viral load at start of treatment • CD4 or CD8 counts of zero • inconsistent data and dates (e.g. HIV+ve date before HIV-ve date, any odd or future dates) • overlapping drug start/stop dates All queries are investigated and both CHIC and clinic databases are updated with corrected information
De-duplication process Individuals may have attended more than one clinical centre. Potential matches identified by matching date of birth and soundex; other demographic variables are used to determine whether potential matches are definite or indeterminate, e.g. - HIV+ve dates in same calendar year - dates of death within 1 month - transferred to/from same centre - first/last seen dates are consistent - same country of birth (non-UK only) Once duplicate patients have been identified, data from individual records are combined.
Improving death data • Many patients do not ‘reappear’ at their clinics for long periods of time; some of these may have left the country and/or may have died. • UK CHIC records are matched to records held at the PHE (which include death data from the Office of National Statistics) • Matches are sent to centres to check that no evidence exists that the patient is still alive; when confirmed, the database is updated.
Audit of data • 1% of records from each centre are audited. • Each record ‘recreated’ using data obtained from clinical notes and compared with information stored on database (not CD4 or viral load). • Exact match required for demographic data, and date to within 1 month for dates of starting ART and AIDS events. • Demographic data generally reasonable (a few problems with ethnicity and country of birth); some discrepancies in AIDS events or dates. • Some AIDS events and ARV drugs found in notes but not database and vice versa.
Link to UK HIV Drug Resistance Database • UK CHIC is linked with UK Collaborative Group on HIV Drug Resistance, set up in 2001 to collect information on routinely performed resistance tests in the UK. • Resistance test data (sequences) are collected. • There is substantial overlap of patients in the two databases so clinical information is shared. • Results of over 106,000 resistance tests relating to 66,100 patients are stored on the database – 24,700 patients have linked clinical data in the UK CHIC study (data to end of 2012).
Characteristics of cohort CHIC 2013 dataset
Collaborations TDM Registry University of Liverpool Collaborative HIV Paediatric Study (CHIPS) European COHERE collaboration UK HIV Drug Resistance database National Study of HIV in Pregnancy and Childhood (NSHPC) Statistical research/ methodology groups Public Health England (surveillance)
Acknowledgements • Steering Committee: • Jonathan Ainsworth, Sris Allan, Jane Anderson, Abdel Babiker, David Chadwick, Valerie Delpech, David Dunn, Martin Fisher, Brian Gazzard, Richard Gilson, Mark Gompels, Phillip Hay, Teresa Hill, Margaret Johnson, Sophie Jose, Stephen Kegg, Clifford Leen, Fabiola Martin, Mark Nelson, Chloe Orkin, Adrian Palfreeman, Andrew Phillips, Deenan Pillay, Frank Post, Jillian Pritchard, Caroline Sabin (PI), Memory Sachikonye, Achim Schwenk, Anjum Tariq, John Walsh. • Central Co-ordination: Teresa Hill, Sophie Jose, Andrew Phillips, Caroline Sabin, Alicia Thornton, Susie Huntington (UCL); David Dunn, Adam Glabay (Medical Research Council Clinical Trials Unit [MRC CTU at UCL]) • Participating sites: • Brighton and Sussex University Hospitals NHS Trust(M Fisher, N Perry, S Tilbury, E Youssef, D Churchill); Chelsea and Westminster Hospital NHS Foundation Trust, London (B Gazzard, M Nelson, R Everett, D Asboe, S Mandalia); King’s College Hospital NHS Foundation Trust, London(F Post, H Korat, C Taylor, Z Gleisner, F Ibrahim, L Campbell); Mortimer Market Centre, University College London(R Gilson, N Brima, I Williams); Royal Free NHS Foundation Trust/University College London (M Johnson, M Youle, F Lampe, C Smith, R Tsintas, C Chaloner, S Hutchinson, C Sabin, A Phillips, T Hill, S Jose, A Thornton, S Huntington); Imperial College Healthcare NHS Trust, London (J Walsh, N Mackie, A Winston, J Weber, F Ramzan, M Carder); Barts and The London NHS Trust, London (C Orkin, J Lynch, J Hand, C de Souza); Homerton University Hospital NHS Trust, London(J Anderson, S Munshi); North Middlesex University Hospital NHS Trust, London (J Ainsworth, A Schwenk, S Miller, C Wood); The Lothian University Hospitals NHS Trust, Edinburgh(C Leen, A Wilson, S Morris); North Bristol NHS Trust (M Gompels, S Allan); Leicester,University Hospitals of Leicester NHS Trust(A Palfreeman, K Memon, A Lewszuk); Middlesbrough, South Tees Hospitals NHS Foundation Trust (D Chadwick, E Cope, J Gibson); Woolwich,Lewisham and Greenwich NHS Trust(S Kegg, P Main, Dr Mitchell, Dr Hunter), St George’s Healthcare NHS Trust(P Hay, M Dhillon); York Teaching Hospital NHS Foundation Trust (F Martin, S Russell-Sharpe); Coventry, University Hospitals Coventry and Warwickshire NHS Trust(S Allan, A Harte, S Clay); Wolverhampton, The Royal Wolverhampton Hospitals NHS Trust(A Tariq, H Spencer, R Jones); Chertsey, Ashford and St Peter’s Hospitals NHS Foundation Trust(J Pritchard, S Cumming, C Atkinson);Public Health England, London (V Delpech);UK Community Advisory Board(M Sachikonye). Funding: UK CHIC is funded by the UK Medical Research Council