Download
1 / 64
660 likes | 715 Views
CARCINOMA RECTUM. CARCINOMA OF RECTUM. CARCINOMA OF RECTUM. Second most common visceral tumour of the body Common above 50 yrs Younger age – bad prognosis Male : female – 1.2 : 1. AETIOLOGY. Red meat & saturated fatty acids Alcohol & smoking FAP & adenomas are more prone for carcinomas

E N D
CARCINOMA OF RECTUM • Second most common visceral tumour of the body • Common above 50 yrs • Younger age – bad prognosis • Male : female – 1.2 : 1
AETIOLOGY • Red meat & saturated fatty acids • Alcohol & smoking • FAP & adenomas are more prone for carcinomas • Villous adenoma has 40% chance of turning malignant • Ulcerative colitis, Crohns disease, HNPCC carries higher incidence of carcinoma of rectum • Family history of rectal cancer – any 1st degree relative of a person with rectal cancer will show 2 times increased risk of carcinoma rectum
DIETARY FACTORS • Excess calorie intake • Low content of unabsorbable vegetable fibre • High content of refined carbohydrates • Intake of red meat • Decreased intake of protective micronutrients
PRE-EXISTING DISEASES • INFLAMMATORY BOWELDISEASE ULCERATIVE COLITIS 1% PER YEAR AFTER 10 yrs 10% RISK AFTER 20 yrs CROHNS DISEASE 7% RISK AFTER 20 yrs COLONIC STRICTURES- ADENO CARCINOMA AT THE SITE OF FIBROTIC NARROWING EXCLUDED SEGMENTS AFTER SEGMENTAL BYPASS
HNPCC • Hereditery non polyposis colon cancers 4 – 6 % rectal malignancies • Lynch syndrome 1 - Autosomal dominant -Site specific within family -4% may develop carcinoma
HNPCC Lynch syndrome 2 • Autosomal dominant • Deletion of mismatch repair gene • Colorectal,endometrial, gastric and other types of cancers
ADENOMA – CARCINOMA SEQUENCE • Proposed by vogelstien • Adenocarcinoma develop from pre-existing adenoma
ADENOMA – CARCINOMA SEQUENCE CONTD. • High prevelence adenoma has high prevelence of carcinoma • Distribution of adenoma within the rectum is comparable to that of carcinoma • In case of early invasive ca , sorrounding tissue shows preceding changes of evolution
ADENOMA –CARCINOMA SEQUENCE CONTD • Peak incidence of adenoma antedates by some years the peak of carcinoma rectum • Risk of carcinoma declines with removal of all identified adenomas
ADENOMA –CARCINOMA SEQUENCE CONTD. • RISK OF DEVELOPING CARCINOMA • Number • Size – large • Type – villous component
PATHOLOGY MACROSCOPY • Annular encircling lesions • Central ulcerations with elevated margins • Papilleferous infiltrating type • Early lesions are small button like areas of elevation
MICROSCOPY • 95% are ADENOCARCINOMAS
MICROSCOPY • 10% of these are colloid carcinomas
HISTOLOGY • Well differentiated • Moderately differentiated • Poorly differentiated-anaplastic
SPREAD OF THE CARCINOMA • Local spread • Lymphatic • Haematogenous spread • Peritoneal dissemination
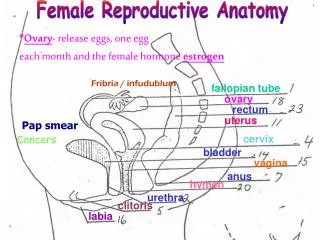
LOCAL SPREAD • ANTERIOR- • IN MALES PROSTATE,BLADDER& SEMINAL VESICLES. • IN FEMALES Uterus , Cervix, Posterior wall of vagina, Pouch of Douglas
LOCAL SPREAD • Posterior sacrum&sacral plexus • Lateral- ureter • Downward- anaplastic carcinoma
LYMPHATIC • Above the peritoneal reflection- to the inferior mesenteric nodes • Below this level to about 1-2cm of the anal orifice is also to the inferior mesenteric nodes • In the field of middle rectal arteries spread along these vessels • Pre aortic,internal illiac and sacral lymph nodes
HAEMATOGENOUS SPREAD • Via the venous system • Anaplastic and rapidly growing tumours • sites .liver- 34% .lungs- 22% .adrenals- 11% .brain,bone,ovary- 33%
PERITONEAL DISSEMINATION • Follow penetration of peritoneal cavity by a high lying rectal carcinoma
CLINICAL FEATURES • BLEEDING • Earliest, common symptom • Fresh bleeding • Blood stained stools • Blood staining the clothing
CLINICALFEATURES • SENSE OF INCOMPLETE DEFECATION • Tenesmus - cancers of lower rectum • Spurious diarrhoea • Bloody slime
CLINICAL FEATURES CONTD Alteration in bowel habit • Early morning bloody diarrhoea • Annular carcinoma- increasing constipatiion • Growth at ampulla of rectum- early morning diarrhoea
CLINICAL FEATURES • PAIN Colicky type- advanced growth at rectosigmoid junction Severe – deep carcinomatous ulcer erodes the prostate or bladder Pain in back or sciatica –sacral plexus
CLINICAL FEATURES • WEIGHT LOSS • ANAEMIA
EXAMINATION • ABDOMINAL EXAMINATION • Normal in early lesions • Advanced growths- signs of large intestinal obstruction, colon loaded with faeces may be felt • Liver palpated for metastasis • Ascites
EXAMINATION PER RECTAL EXAMINATION • Early cases – plateau or a nodule with an indurated base • Centre ulceration – shallow depression with everted raised edges • Finger smeared with blood or mucopurelent material tinged with blood
STAGING OF CANCER Dukes staging • a- growth limited to the rectal wall • b- the growth extended to the extra rectal tissue but no metastasis to regional lymph nodes • c- there are secondary deposits in the regional lymphnodes .c 1- local pararectal lymphnodes alone .c 2- nodes accompanying the supplying vessels d D - presence of wide spread metastasis
STAGING • ASTER COLLER STAGING • A- MUCOSA ONLY • B1- SUBMUCOSA INVOLVED • B2- MUSCULARIS INVOLVED • C1- INVOLVEMENT OF MUSCULARIS AND NODES • C2- INVOLVEMENT OF SEROSA AND NODES • D- DISTANT METASTASIS
TNM STAGING • Tx – Primary tumour cannot be assessed • Tis – Confined to the mucosa • T1 - Extend upto submucosa • T2 – Extends into the muscularis propria • T3 – Extends in to the sub serosa but not to adjacent structures • T4 – Involves adjacent structures
TNM STAGING • Nx – cannot be assessed • N0 – no lymph node metastasis. • N1 – cancer cells found in 1 to 3 nearby nodes • N2 – cancer cells in 4 or more nodes • N3 – cancer cells in nodes along named vessels
TNM STAGING • Mx – distant metastasis. cannot be assessed • M0 – no distant metastasis. • M1 – distant metastasis present
INVESTIGATIONS • Proctoscopy • Sigmoidoscopy • Biopsy • Barium Enema • Colonoscopy • USG abdomen to look for secondaries • CT to check for operability
SURGERIES • ABDOMINO-PERINEAL RESECTION • Wherein sigmoid, descending colon & upper rectum is mobilised per abdomen • Anal canal with perianal & perirectal tissues are dissected per anally • Retained colon is bought out as end colostomy in left iliac fossa
TYPES • MILES – Abdomen first, perineum later • GABRIEL – perineum first, abdomen later • Lloyd Davis – synchronised(combined)
PROCEDURE • APR is done through lower midline incision in lithotomy position • Left sided colon & entire rectum is mobilised from above • Rectum is mobilised posteriorly in avascular plane in front of the nerve plane between mesorectum & sacrum • Inferior mesentric artery is ligated high proximal at its origin or just beyond its first branch
CONTD…. • Colon is transected & proximal cut end is fashioned from end colostomy in left iliac fossa • Through perineum a purse string suture is place around anal margin • Circumferential suture is placed around the anus • Dissection is deepened using scissor & cautery into the perineal body • First posterior & lateral dissections are undertaken, then anterior dissection • Perineal wound is closed in layers,Abdomen drain is placed, colostomy is created
COMPLICATIONS • Bleeding • Infection of perineal wound • Complications of colostomy like prolapse, stenosis & infection • Injury to urinary system, ureter, impotence, urinary incontinence
Sphincter Saving APR with Colo-Anal Anastamosis • Done in operable distal rectal tumor in young individual • Here permanent colostomy is avoided
ANTERIOR RESECTION • Also called anterior procto-sigmoidectomy through abdominal approach wherein rectum above peritoneal reflection is resected with colorectal anastamosis • Done in growths in the mid & upper parts of the rectum
LOW ANTERIOR RESECTION • CRITERIA • Upper & middle third growth • Above peritoneal reflection • Well differentiated tumor • < 4cm in size tumor • In females growth 7 cm above the anal verge • T1 N0/T2 N0 tumor • Tumor without lymphatic or venous spreas
ADVANTAGES OF LAR • Avoids permanent colostomy • Sphincter retained • Patients acceptance DISADVANTAGES • Uncertainity of clearance • Anastamotic leak, infection, stenosis
HARTMANN’S OPERATION • Palliative procedure • Done in elderly people not fit for major surgery • Here rectal growth is resected & upper end of rectum is closely approximated • Proximal colon is brought out as end colostomy
RADIOTHERAPY • Only rectal carcinoma in GIT responds well to RT • Pre- op RT can be given to downstage the tumor • Intra-operative RT is used in pelvic wall disease • Short course 25GY in 5 fractions in 5 days • Long course 5040 Gy in 28 fractions in 6 weeks
CHEMOTHERAPY • Drugs like Endoxan, 5 FU, semustine also with leucovarine • Capecitabine & oxaloplatin are newer drugs • Biological Agents- - Bevacizumab VEGF receptor antagonist - Cetuximab EGFR antagonist
RECTAL PROLAPSE • Circumferential descent of rectum through the anal canal • Commonly seen in infants, children & elderly individuals • Common in females (6:1)
Rectal prolapse can be : • Partial • Complete • Hidden/Concealed – internal intussusception of the sigmoid into the rectum distally, they do not come out of the anal orifice.Here only mucosa & submucosa separates from muscularis layer & descends
AETIOLOGY • Decreased sacral curvature & decreased anal canal tone are the probable causes in infants • Chronic constipation with straining is the common cause • Diarrhoea, cough & malnutrition • Reduced ischiorectal fossa fat • Pudendal nerve damage pelvic floor & anal canal weakness • In adult females- repeated birth injuries in the perineum results in damage to perineal nerve supply





![STOMACH, INTESTINES, RECTUM [SURGICOSE]](https://cdn4.slideserve.com/8061806/medical-instruments-medical-instruments-dt.jpg)