Download
1 / 56
560 likes | 585 Views
Learn how Premier Inc. partners with healthcare systems to improve community health and reshape healthcare. Explore quality measures and the future of healthcare quality.

E N D
CMS/Premier Hospital Quality Incentive Demonstration Project Health Insurance Review Agency - Symposium November 8, 2005 Stephanie Alexander, MBA Senior Vice President, Premier Inc. General Manager, Premier Healthcare Informatics Charlotte, North Carolina, USA
Owners Affiliates Premier, Inc. • Private organization; owned by more than 200 not-for-profit health systems • Customer base of more than one-third of the United States hospitals Core Purpose: To improve the health of communities. Envisioned Future:“Premier’s owners will be the leading healthcare systems in their markets, and, with them, Premier will be a major influence in reshaping healthcare.” (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Envisioned Future (cont.): Premier hospitals and health systems ‘will operate at costs in the lowest quartile… and at quality levels in the highest quartile…’ What we do and why we do it (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Premier Healthcare Informatics (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Centers for Medicare andMedicaid Services • CMS is a agency within the United States Department of Health and Human Resources • Medicare – healthcare services for the elderly • Medicaid – healthcare services for the poor • Finances over half of the United States healthcare costs • Funds demonstration projects mostly requested by US Congress prior to full program launch Typical USA Acute Care Hospital Payer Mix (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Pressure for better value • The profession • Institute of Medicine Reports • Business health coalitions • Leapfrog Group • Midwest Business Group on Health • Pacific Business Group on Health • Washington Business Group on Health • Consumerism • Healthgrades.com • Quality “scorecard” movement • JCAHO-ORYX • NCQA-HEDIS • Quality “Awards” (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
The quality imperative Only 45% of patients experiencing a heart attack received beta-blockers and only 61% were advised of aspirin therapy “Only half (54.9%) of patients received the recommended care for their illness or injury..” RAND Corporation Study, 2003 (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Heart Failure Efficiency and Effectiveness Percentile Comparisons Premier Perspective Comparative Database: 3Q01 - 2Q02 Top Decile 100.00% 90.00% 80.00% 70.00% 60.00% (Wage/Severity Adjusted Cost and Severity Adjusted ALOS) Efficiency 50.00% 40.00% 30.00% 20.00% 10.00% 0.00% 0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00% 90.00% 100.00% Effectiveness Percentile Bottom Decile (Risk Adjusted Mortality, Readmissions, ACE Inhibitor Use) Unwarranted variation (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Quality movement here to stay • Quality movement in other industries decades old, still going strong. • Six Sigma • ISO 9000 • Malcolm Baldrige Award of Quality • Healthcare only starting to adopt these standards • Only four healthcare Baldrige winners during past three years (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
What is it going to take to get better in quality? • Quality of care must be measured routinely at the national and provider level • Transparency of quality measures • Must address the fact that current financial incentives are not aligned with quality improvement • Must create a culture of quality in all hospitals and health systems (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
How do we measure quality? • Clinical quality measures include both process and outcome indicators • Process indicators focus on key activities that evidence suggests are critical to improved outcomes • Beta blockers within a prescribed timeframe • Administration of antibiotics • Outcome indicators focus on the end result of treatment • Risk-adjusted mortality • Readmission rates • Patient satisfaction • Safety measures (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
How do we measure quality? • No single measure is perfect, but we have to start somewhere • Example: • Hospital mortality Institute of Healthcare Improvement (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
How do we measure quality? • Quality indicators are typically identified by consensus of many clinicians and organizations, based on clinical evidence • Physician associations • National Quality Forum (NQF) • Agency for Healthcare Research and Quality (AHRQ) • CMS 7th Scope of Work • JCAHO Core Measures • The Leapfrog Group • Premier Clinical Focus Groups (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
What is it going to take to get better in quality? • Quality of care must be measured routinely at the national and provider level • Transparency of quality measures • Must address the fact that current financial incentives are not aligned with quality improvement • Must create a culture of quality in all hospitals and health systems (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Transparency Transparency of quality data is essential to spread quality improvement… Don Berwick, M.D., President, Institute of Healthcare Improvement Transparency of performance for hospitals, doctors, and other medical institutions is a first step to creating a quality strategy. While we are beginning to move in this direction, the pace of progress is slow. Margaret E. O’Kane, President of the National Committee for Quality Assurance (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Consumer information CMS Annual Payment Program Outgrowth of a National Voluntary Hospital Reporting Initiative • “Starter set” of 10 measures • Heart Failure, AMI, Pneumonia • Underlying data is reliable • Hospitals that do report do not receive Medicare rate increases • “Pay for reporting” program (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
“P4P” What is it going to take to get better in quality? • Quality of care must be measured routinely at the national and provider level • Transparency of quality measures • Must address the fact that current financial incentives are not aligned with quality improvement • Must create a culture of quality in all hospitals and health systems (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Thomas Scully Former Administrator, Centers for Medicare and Medicaid Services, 2003 “I don’t think it makes a lot of sense to pay every hospital in Boston exactly the same amount for a hip replacement regardless of their quality, but we are.” Mark McClellan, M.D., Ph.D. Administrator, Centers for Medicare and Medicaid Services, 2004 "Our goal at Medicare is to stimulate care that is efficient and effective for every patient. The Premier/CMS demonstration, and others that are a part of the new Medicare law, will help us work with providers to improve the quality of care that our beneficiaries receive." Premier/CMS HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Why we need pay for performance “At issue is not the dedication of health professionals but the lack of systems . . . that reduce errors and reinforce best practices. We have concluded that such systematic changes will not come forth quickly enough unless strong financial incentives are offered to get the attention of managers and governing boards.” “Our recommendation . . . is that payment for performance should become a top national priority. We should settle for nothing less.” Health Affairs, November/December 2003; Open letter signed by 15 leaders of the quality movement, including seven physicians (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
First national “pay for quality” effort “Groundbreaking . . . Pay for performance should become a top national priority” - Open letter in Health Affairs signed by 15 leaders in the quality movement. “I would like to see 5,000 hospitals participating.” - Tom Scully in Modern Healthcare “Fix For a Sick System” - InformationWeek 9912235090093230991345348729847 99994500900900909874987496592659275028529 99994500900900909508749856249861741034871093741037 09091769846198641641340198923438430438 (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Performance Group Lowest Top Performers Performance Innovation Group Opportunity Group Hospitals Bottom quartile in performance (high cost, low quality) Top decile in performance (low cost and high quality) Is there a business case for quality in hospitals? (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CABG Performance Source: Premier PerspectiveTM (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Non-collaborators’ financial performance Source: Premier PerspectiveTM (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Collaborators’ financial performance Source: Premier PerspectiveTM (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Non-collaborators’ clinical performance Source: Premier PerspectiveTM (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Collaborators’ clinical performance Source: Premier PerspectiveTM (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Program Introduction CMS/Premier Hospital Quality Incentive (HQI) Demonstration Project • The first national project to measure hospital performance and offer additional Medicare payment for top quality care • “Pay for quality” • Can economic incentives effectively improve quality of care? CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Program Overview • A three-year effort linking payment with quality measures (launched October, 2003) • Top performers identified in five clinical areas • Acute Myocardial Infarction • Congestive Heart Failure • Coronary Artery Bypass Graft • Hip and Knee Replacement • Community Acquired Pneumonia Indicators within AMI, CABG, HF, and CAP represent all patients (all payers). Hip and knee replacement indicators apply only to Medicare patients. CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI - National participationOver 260 participating hospitals CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Identifying Top Performers • Composite Quality Index will identify hospitals performing in the top two deciles in each clinical focus group • Composed of two components: • Composite Process Rate • Risk-Adjusted Outcomes Index • Clinical conditions without outcomes indicators use only the Composite Process Rate CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
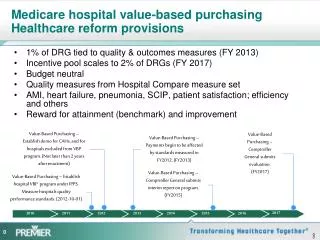
Payment Overview • “Top Performers” are defined annually as those in the first and second decile • Incentive payment threshold changes each year per condition • Top decile performers in a given clinical area receive a 2 percent Medicare payment supplement per clinical condition • Second decile performers receive a 1 percent Medicare payment supplement per clinical condition. CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Condition X Condition X Payment Incentive Condition X + 2% 1st Decile 2nd Decile Payment Incentive 1st Decile 3rd Decile Payment Incentive 4th Decile 1st Decile 2nd Decile Top Performance Threshold 5th Decile 3rd Decile 6th Decile 2nd Decile 4th Decile 7th Decile + 1% 5th Decile 8th Decile 3rd Decile 9th Decile 6th Decile 4th Decile 10th Decile 7th Decile Hospital 5th Decile 8th Decile 9th Decile 6th Decile 10th Decile 7th Decile Payment Adjustment Threshold Hospital 8th Decile - 1% 9th Decile 10th Decile - 2% Year One Year Two Year Three Payment Adjustment - Year 3 Anticipated payment scenario CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Transparency in measures The CMS/Premier quality measures are based on clinical evidence and industry recognized metrics with standardized definitions from: • All 10 indicators from the National Voluntary Hospital Public Reporting Initiative • 27 indicators from the National Quality Forum (NQF). • 24 indicators from CMS 7th Scope of Work. • 15 indicators from JCAHO Core Measures. • 3 indicators proposed by The Leapfrog Group. • 4 indicators from the Agency for Healthcare Research and Quality’s (AHRQ) patient safety indicators (2 PSIs applied to 2 clinical populations). CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Transparency in reporting • Public reporting • Top 50% of participants by clinical area • No rankings • Individual indicator values, not overall score • First reporting November 2005 • Frequency: every 6 to 12 months, thereafter • Reporting within the group • In most cases, fully transparent – knowledge transfer CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Current Progress:HQI Results to Date (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI ProjectAlready showing significant improvement (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI ProjectReduction in variation and improvement trend (AMI) (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Large Health SystemParticipants Versus Non-Participants (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Clinical quality indicators • 1 National Quality Forum measure • 2 CMS 7th Scope of Work measure • 3 JCAHO Core Measure • 4 The National Voluntary Hospital Reporting Initiative (AHA Initiative) • 5 The Leapfrog Group proposed measure • 6 Risk adjusted using JCAHO methodology • 7 Risk adjusted using 3M™ All Patient Refined DRG methodology • 8 AHRQ Patient Safety Indicators and risk adjusted using AHRQ methodology. • 9 Medicare beneficiaries only • 10 CMS and/or JCAHO to align with this measure in 2004 • 11 Surgical Infection Prevention (SIP) measure • P Process measure • O Outcomes measure CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Clinical quality indicators CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Clinical quality indicators CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Clinical quality indicators CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Clinical quality indicators CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Key to Quality Improvement • “Quality” core value of institution • Priority of executive team • Physician engagement • Improvement methodology • Prioritization methodology • Dedicated resources • Committed “knowledge transfer” CMS/Premier HQI Demonstration Project (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE
Premier Rapid Improvement Guides (c) 2005 By Premier, Inc. PROPRIETARY AND CONFIDENTIAL - DO NOT COPY OR DISTRIBUTE