Download
1 / 4
40 likes | 105 Views
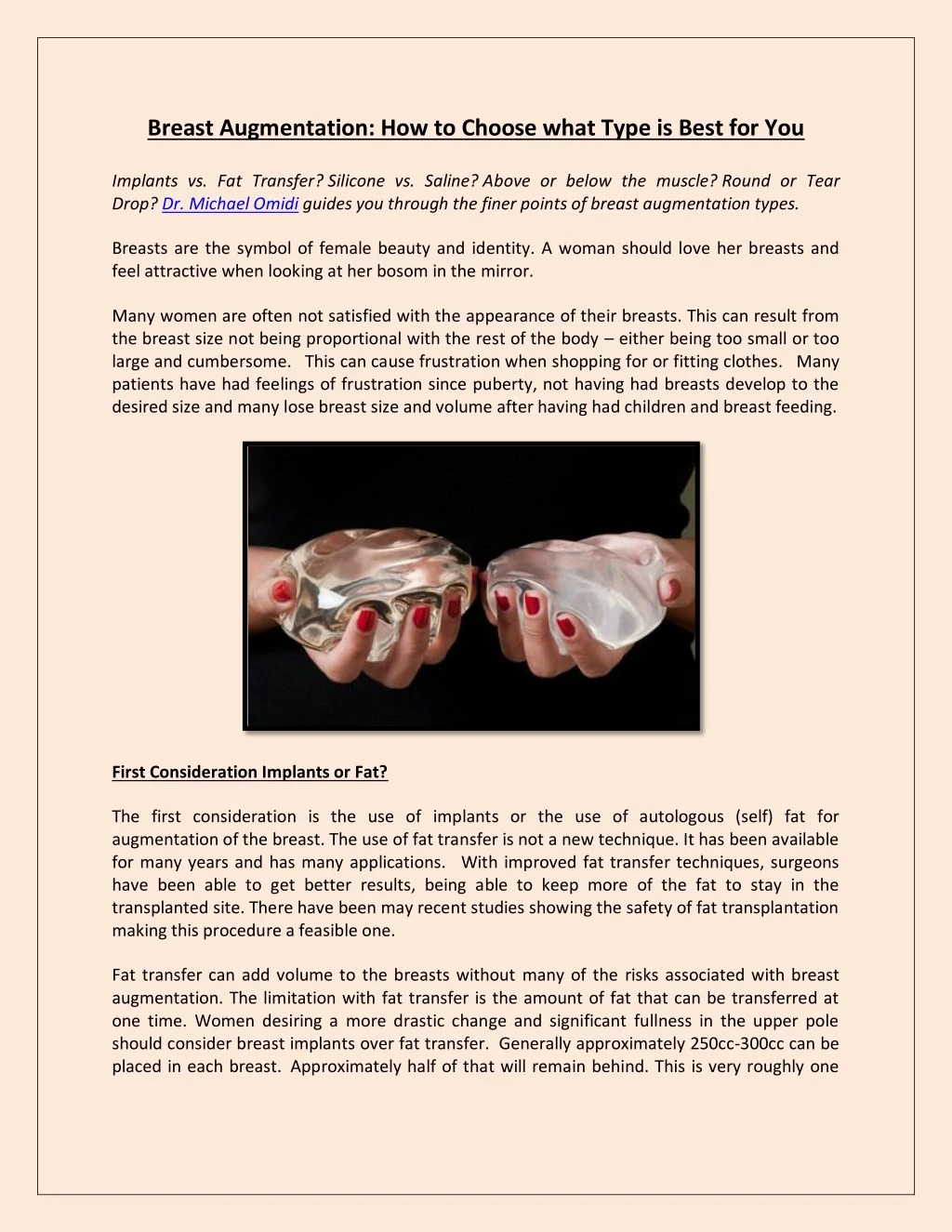
Implants vs. Fat Transfer? Silicone vs. Saline? Above or below the muscle? Round or Tear Drop? Dr. Michael Omidi guides you through the finer points of breast augmentation types.<br>

E N D
Breast Augmentation: How to Choose what Type is Best for You Implants vs. Fat Transfer? Silicone vs. Saline? Above or below the muscle? Round or Tear Drop? Dr. Michael Omidi guides you through the finer points of breast augmentation types. Breasts are the symbol of female beauty and identity. A woman should love her breasts and feel attractive when looking at her bosom in the mirror. Many women are often not satisfied with the appearance of their breasts. This can result from the breast size not being proportional with the rest of the body – either being too small or too large and cumbersome. This can cause frustration when shopping for or fitting clothes. Many patients have had feelings of frustration since puberty, not having had breasts develop to the desired size and many lose breast size and volume after having had children and breast feeding. First Consideration Implants or Fat? The first consideration is the use of implants or the use of autologous (self) fat for augmentation of the breast. The use of fat transfer is not a new technique. It has been available for many years and has many applications. With improved fat transfer techniques, surgeons have been able to get better results, being able to keep more of the fat to stay in the transplanted site. There have been may recent studies showing the safety of fat transplantation making this procedure a feasible one. Fat transfer can add volume to the breasts without many of the risks associated with breast augmentation. The limitation with fat transfer is the amount of fat that can be transferred at one time. Women desiring a more drastic change and significant fullness in the upper pole should consider breast implants over fat transfer. Generally approximately 250cc-300cc can be placed in each breast. Approximately half of that will remain behind. This is very roughly one
extra cup size. It’s not a drastic difference, but often time’s patients are not looking for such – simply a fuller, prettier self. How do we select implants? 1.The first decision to make is Silicone Gel vs. Saline: After having made decision to go forward with implants, the main question of silicone vs saline is posed. My patients often ask me which is better, which is safer and which I recommend. These are all legitimate questions regarding the choice of breast augmentation with implants. I prefer silicone implants because they are softer, thicker and have less rippling. They are a bit costlier than saline implants, approximately double the price. It is important to differentiate the new silicone (cohesive gel implants) from the old liquid silicone implants that were made in the 80’s and early 90s that had many problems from leakage and scarring. The new cohesive gel silicone gel implant are made to maintain consistency to minimize leak, using the term “cohesive.” Cutting through one of these implants is similar to cutting through jello or a gummy bear. This has for the most part eliminated the problems of leakage that plagued the old silicone implants. Many studies have been performed showing safety of the implants. Ongoing long term studies are being conducted to confirm long term safety. The use of silicone gel implants have become a viable option for breast augmentation. 2.Silicone Gel Implant Advantages Cohesive silicone gel implants are softer, thicker and more natural feeling compared to saline implants. Silicone implants have more“give” than saline implants, particularly when laying on the abdomen. The cohesive gel implants are pre-filled and risk of leak is reduced significantly compared to saline. The FDA has, however, recommended routine surveillance with an MRI to confirm that there is no leakage. This can be a down side because MRI imaging is expensive and insurances may not cover the test for cosmetic surgery. Saline implants have a higher risk of leak, approximately 9% lifetime risk overall. Generally larger incisions need to be made for silicone implants since they are pre- filled. Saline implants are empty and are filled after they are placed in the chest pocket. 3.Saline Implant Advantages Saline implants have a long term safety record which new cohesive gels do not. The primary reason is that cohesive gel implants have not been around as long as saline implants and haven’t had the chance to develop a long term safety record yet. Saline implants are approximately half the price or silicone implants.
Since saline implants can be filled after being placed in the pocket, it allows them to be placed from incisions from the armpit (axilla) and umbilicus. 4.Fat Transfer Advantages No foreign body (no implant) No significant incisions or dissection No risks associated with breast implants – hardening (capsular contracture), infection, removal of implants, no injury to the pectoralis muscle. Patients own tissue, natural softer feel 5.Above vs. Below the Muscle: Implants are generally placed under the muscle (submuscular) for multiple reasons. Going under the muscle provides a layer of tissue that protects the implant, reduces visible rippling that is present in all implants and in some studies has shown to reduce the risk of capsular contracture. Implants above the muscle (subglandular) have more visible rippling and often add to the weight of the breast tissue. This results in excess unsupported weight on the breast tissue which can cause premature ptosis (sagging of the breast). I generally reserve placement of an implant above the muscle in select patients that are desiring a small implant, have a tight pocket (not a large amount of loose skin). . Some have advocated placement of the implant above the muscle to fill out loose skin. I have found that this benefit is only a short lasting one, often resulting in additional loose skin over several years time from the additional unsupported weight of the implant on the already thinned and ptotic (sagging) skin. Some physicians use the term biplane or dual plane placement of implants. This term implies that the implant is partially under the muscle and partially under the breast tissue. This is a more descriptive term, but exactly the same position as below the muscle or submuscular positioning. It is more descriptive since the implant is not 100% under the pectoralis muscle. The pectoralis muscle will cover only about half of the implant if the anatomical shape of the muscle in relationship to the chest wall is considered. Complete submuscular breast augmentation is rarely if ever performed for cosmetic breast augmentation. It is more commonly used for breast reconstruction after full mastectomy where the upper half of the implant is placed under the pectoralis muscle and the lower half is placed under the serratus anterior muscle. 6.Shaped vs Round Implants There was a time when shaped implants had become popular for those desiring natural appearing or tear-drop shaped breasts. The implants were shaped like a tear drop to achieve a more natural look. These implants are rarely used today. They create more of a wild card then
achieving their purpose. A “more” natural breast can be achieved by minimizing the size of the implant placed in the pocket. The round shape adds the volume necessary Final Recommendations: After considering the advantages and disadvantages. If a patient is looking for a very subtle improvement and does not want to undergo incisions, dissection and the risks of implants, fat transfer is an excellent option. For ladies that want a more significant change in the appearance of the breast, then an implant is a better option. I usually recommend silicone gel implants unless the budget is restricted. I also usually recommend the periareloar approach (incision around the areeola). My second choice is the inframmary incision which is under the breast. The scar is somewhat more visible when looking at the underside of the breast. Some women prefer the nipple to be untouched. However, I have found that the scar around the nipple is less visible camouflaging on the border of the areola and breast skin. The thinner areola skin also results in a less visible scar. Silicone gel implants though softer, are about twice the price of saline implants, require a larger incision and the FDA has now recommended MRI screening every two years. The patient can make the final choice based on the advantages and disadvantages listed above. Both are excellent options. This site is not designed to and does not provide medical advice, professional diagnosis, opinion, treatment or services to you or to any other individual. Through this site and linkages to other sites, Dr.Michael Omidi or affiliates provides general information for educational purposes only. The information provided in this site, or through linkages to other sites, is not a substitute for medical or professional care, and you should not use the information in place of a visit, call consultation or the advice of your physician or other healthcare provider. Dr.Michael Omidi or affiliates is not liable or responsible for any advice, course of treatment, diagnosis or any other information, services or product you obtain through this site.