Download
1 / 10
110 likes | 409 Views
Acute Appendicitis Tintinalli Ch 84. Pathophysiology. Obstruction of appendiceal lumen Food matter, Adhesions, Lymphoid hyperplasia, Mucosal secretion Causes increased intraluminal pressure Vascular compromise Causes breakdown of epithelial mucosa and bacterial invasion

E N D
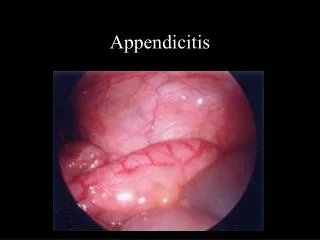
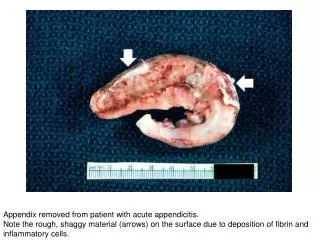
Pathophysiology • Obstruction of appendiceal lumen • Food matter, Adhesions, Lymphoid hyperplasia, Mucosal secretion • Causes increased intraluminal pressure • Vascular compromise • Causes breakdown of epithelial mucosa and bacterial invasion • Inflammatory response • Eventually leads to arterial stasis and tissue infarction
Innervation • Luminal distention triggers visceral afferent fibers entering at T10 → Vague, poorly localized periumbilical or epigastric • Inflammation of serosa localized to RLQ • Anatomic Variability • Retrocecal (26%) → Flank Pain • Pregnant Women → RUQ Pain • Retroileal → Testicular Pain • Pelvic → Irritate bladder/rectum, suprapubic pain/pain with urination/defecation
Symptoms • Vague abdominal pain with localization -64% sensitive, 82% specific • Anorexia - 68% sensitive, 36% specific • N/V - 50% sensitive, 45% specific • Rebound tenderness - 63% sensitive, 69% specific • Guarding - 74% sensitive, 57% specific • Rigidity - 27% sensitive, 83% specific • Fever - 67% sensitive, 79% specific
Physical Exam • McBurney’s point • May have rectal or flank tenderness if pelvic or retrocecal • Rovsing sign - Palpation of LLQ produces RLQ pain • Psoas sign - Patient in left lateral decubitus, Extend right leg at hip • Obturator sign - Passive flexion of hip & knee with internal rotation of hip
Diagnostics • CBC 70-90% sensitive, low specificity • Urinalysis - Abnormal in 19-40% • Plain Radiographs - Limited diagnostic value • Abnormal in 24-95% • Look for appendiceal gas, fecalith, localized paralytic ileus, blurred right psoas muscle, free air
Diagnostics • Graded Compression Ultrasound – Test of choice in children and pregnant women • 94.7% sensitive, 88.9% specific • Inflamed appendix cannot be compressed • Findings • Diameter > 6mm • Presence of appendicolith • Periappendiceal abscess • Doppler may show hyperemia • Limitations • Retrocecal • Ruptured appendix = normal diameter
Diagnostics CT – Contrast may not be necessary, depends on your radiologist Findings • Pericecal inflammation • Abscess • Periappendiceal phlegmon • Fluid collections • Localized fat stranding
Special Populations • Very young, High misdiagnosis rate, High perforation rate, Communication difficulty • Atypical symptoms • Concurrent respiratory symptoms • Gastroenteritis • Lethargy, inactivity, hypothermia • Elderly, Late presentation with an advanced course, Misdiagnosis can exceed 50%, Incidence of perforation 40-70%, Mortality rate in patients > 70 ~ 30% • Pregnant • Most common extrauterine surgical emergency • Fetal mortality rate increases up to four times if complicated by perforation and peritonitis
Management • NPO • IV fluids • Preoperative antibiotics cover for anaerobes, enterococci, and gram-negative’s • Zosyn or Unasyn • Analgesics • Surgical consult