Download
1 / 21
410 likes | 1.29k Views
ACUTE APPENDICITIS. Presented by : Sara Shokri Moghaddam. Anatomy & Function of appendix. The three taeniae coli converge at the junction of the cecum with the appendix. The tip of appendix can be found in a retrocecal,pelvic,subcecal,preileal or right pericolic position.

E N D
ACUTE APPENDICITIS Presented by : Sara ShokriMoghaddam
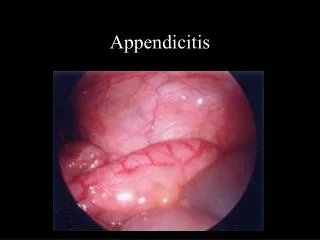
Anatomy & Function of appendix • The three taeniae coli converge at the junction of the cecum with the appendix. • The tip of appendix can be found in a retrocecal,pelvic,subcecal,preileal or right pericolic position.
Anatomy & Function of appendix • Appendix is an immunologic organ that participate in the secretion of IGs., specially IgA.
Incidence • ≈ 7 % of all people andergoes appendectomy during their life • More frequently in 2nd through 4th decades of life • M > F • The percentage of misdiagnosed cases of appendicitis is higher among women.
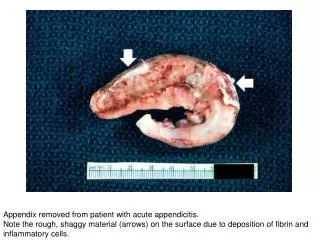
Etiology and Pathogenesis • Obstruction of the lumen is the dominant etiologic factor of appendicitis. • The most common cause of obstruction is fecaliths. • Other causes:hypertrophy of limphoidtissue,inspissatedbarium,tumor,vegetable and fruit seeds and intestinal parasites.
Etiology and Pathogenesis • A sequence of events lead to appendicitis: Proximal obstruction and normal secretion of mucosa Distention of appendix Stimulation of visceral afferent nerves a vague diffused pain in the midabdominal or lower epigastrium
Distention of appendix N/V occlusion of capillaries vascular congestion involvement of the serosa involvement of parietal peritoneum SHIFT in the PAIN to RLQ
Bacteriology • The bacterial population of a normal appendix is similar to that of normal colon • The principal organisms seen in the normal appendix,in acute appendicitis, and in perforated appendicitis are Escherichia coli & Bactroidfragilis.
AB prophylaxis • Effective in prevention of wound infection and abcesses. • 24-48h in non perforated appendicitis. • 7-10D in perforated appendicitis.
Clinical manifestations SYMPTOMS: • Abdominal pain • Shifting of pain to the RLQ • Anorexia • N/V • Sequence of symptoms: anorexia pain N/V(if accours)
Clinical manifestations SIGNS: • Tendernes around Mcburney point • Rebound tenderness • Rovsing sign • Guarding • Obturator sign • Psoas sign
Laboratory findings • Mild leukocytosis (10000 to 18000) • Several RBC or WBC can be present from ureteral or bladder irritation
Imaging studies • Plain films of the abdomen • Barium enema examination and radioactively labeled leukocyte scans • Compression sonography • High resolution helical CT
Differential Diagnosis • Acute mesenteric adenitis • PID • Ruptured graffian follicle • Twisted ovarian cyst • Ruptured EP • Acute gastroentritis • Meckle’s diverticulitis • Crohn’sentritis • Colonic lesions • Other diseas
Treatment • Open appendectomy • Laparoscopic appendectomy • Natural orifice transluminatiom endoscopic surgery • Antibiotics • Interval appendectomy
Incidental appendectomy • Childrens about to undergo chemotherapy • Disabled patient • Patients with crohn’s disease • The indivisual who are about to travel to remote places