Download
1 / 44
440 likes | 675 Views
Trial Design Issues in SLE. Joel Schiffenbauer FDA/CDER DAAODP. SLE. SLE may wax and wane with and without therapy making determination of the efficacy and safety of new therapies difficult

E N D
Trial Design Issues in SLE Joel Schiffenbauer FDA/CDER DAAODP
SLE • SLE may wax and wane with and without therapy making determination of the efficacy and safety of new therapies difficult • Use of potentially toxic medications requires rigorous study design to demonstrate clear evidence of efficacy and safety (risk/benefit)
Trial Design Issues • Choice of endpoints • Data to collect • Controls and trial designs/SOC issues • Blinding • ITT analysis/Imputation of missing data • Stratification • Covariates • Concomitant medications
Efficacy Trial Considerations • Design will depend on claims sought • Endpoints • Organ specific • Constitutional manifestations/ signs and symptoms • Flare • Other: surrogates, steroid dose
Disease activity • Active • treated vs untreated • Inactive (or relatively inactive) • treated vs untreated
Endpoints • Active disease • disease activity measures (indices; organ specific) • responder index (eg disease activity measure+HRQOL+damage+steroid dose etc) • steroid dose/concomitant medications dose • Inactive disease • flare (time to, number of, rate of) • steroid dose/concomitant medications
Endpoints • What changes are considered clinically meaningful? • What constitutes a successful outcome?
Flares • What reduction in flare rate is clinically meaningful in the context of adverse events? • Are all flares equal (renal vs joints)? • Should a new therapy be asked to address the treatment of active disease in addition to preventing flares?
Advantages and Disadvantages of Flare Design • Advantages • “Responder analysis” takes into account individual responses • Reduces time of partial treatment • Disadvantages • “Heterogeneous” outcomes • Does not demonstrate treatment of active disease • Impractical (few flares)
Examples of Organ Specific Flare Definition • Renal flare: attributed to SLE by treating physician (one or more criteria?) • reproducible increase in serum creatinine greater than 20% accompanied by proteinuria, hematuria and/or RBC casts and /or WBC casts; • Reproducible increase in 24 hour protein (how much?)
General Flare Definition • Defined as at least one of the following: • increase in prednisone (>5mg/day) for at least 14 days since the previous visit • SLE manifestation requiring hospitalization • addition of new medication or an increase in the dose of an existing medication to specifically treat a manifestation of increased SLE activity
Trial Design Issues • Choice of endpoints • Data to collect • Controls and trial designs/SOC issues • Blinding • ITT analysis/Imputation of missing data • Stratification • Covariates • Concomitant medications • Randomization/Allocation concealment
Domains (OMERACT)Lupus 2000; 9:322 • Disease activity measures • SLEDAI, SLAM, BILAG, ECLAM, SELENA SLEDAI, SLAM-R • Definitions of Active Nephritis by U/A, 24 hour CCr, proteinuria • Renal flare • Damage: ACR/SLICC Damage Index • Deterioration of Renal Function: • End Stage Renal Disease [ESRD] • Doubling of Serum Creatinine • Chronicity Index on Biopsy • Health status/HRQOL: SF-36 • Should also include: • Economic costs • Adverse events
Data for Lupus Nephritis • Renal pathology; does everyone need a biopsy? • Urine protein- what is a clinically meaningful change in proteinura? • Urine sediment-what is a clinically meaningful change in hematuria? • Renal function • Serum creatinine • An appropriate measure of GFR-does a change in GFR (vs doubling of serum creatinine) represent an important benefit? • Other: adverse events
Data For Other Manifestations • What data is needed for trials in CNS lupus? • Other manifestations?
Trial Design Issues • Choice of endpoints • Data to collect • Controls and trial designs/SOC issues • Blinding • ITT analysis/Imputation of missing data • Stratification • Covariates • Concomitant medications
Trial Design Informationhttp://www.fda.gov/cder/guidance • ICH E9: Statistical principles for clinical trials • ICH E10: Choice of control group and related issues in clinical trials • RA guidance • SLE guidance (future) • CONSORT (Consolidated Standards of Reporting Trials) recommendations (Lancet 2001; 357:1191)
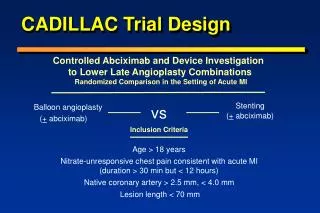
Controls • Ideally a study would have placebo (eg SOC plus placebo vs true placebo) plus active control plus dose response • Allows for measure of absolute effect size • Shows existence of effect • Shows dose response • Allows comparison of therapies
Controls • Superiority trial • SOC (eg steroids plus cyclo) plus new drug vs SOC plus placebo (“add-on” trial) • See Arth. Rheum. 2003; 48:1481 • SOC (eg steroids) plus new drug vs SOC plus cyclo • Equivalence (non-inferiority) • SOC plus new drug vs SOC plus comparator
Other Designs • Limited placebo (steroids only?) period • depends on organ studied • at the beginning of an active control trial (to establish assay sensitivity) • Are there instances where steroids only are an acceptable treatment in lupus nephritis?
Randomized Withdrawal • Subjects receive test treatment for specified time are randomly assigned to continued treatment with the test treatment or placebo • See NEJM 1991; 324:150
Replacement Study • New drug or placebo added by random assignment • conventional treatment given at an effective dose • and the conventional treatment is then withdrawn usually by tapering • Ability to maintain patients baseline status (preventing flares) • Steroid sparing agents
Is There a SOC? • Depends on the organ studied • For lupus nephritis • Are there instances where steroids only are acceptable? • For CNS • For other organ involvement • If cyclophosphamide is used, it may be difficult to demonstrate an effect of the new therapy especially if mechanisms of actions are similar
“Add-on” Trials • Definition of partial responders • Toxicity of combination • Consider factorial design • See also Arth. Rheum. 2003; 48:1481-1483
Equivalence or Non-inferiority Trials • Historical evidence of sensitivity to drug effects based on prior placebo controlled trials • Appropriate trial conduct • setting a margin of difference (cannot be greater than the smallest effect size that the active drug would be reliably expected to have compared with placebo)
Trial Design Issues • Choice of endpoints • Data to collect • Controls and trial designs/SOC issues • Blinding • ITT analysis/Imputation of missing data • Stratification • Covariates • Concomitant medications
Blinding • Blinding is intended to minimize the potential biases resulting from differences in management of patients or interpretation of results • Can trials with IV cyclophosphamide be adequately blinded? Changes in labs, hair loss, nausea • Ann. Int. Med 1971; 75: 165- “therapist” and “observer” (do not know WBC, clinical status); pharmacist to prepare meds; wigs for patients
Why Blind? • Subjects on active drug might report more favorable outcomes because they expect a benefit or might be more likely to stay in a study • Knowledge of treatment could affect the vigor of attempts to obtain on-study follow up
Blinding cont’d • Knowledge of treatment could affect decisions about whether a subject should remain on treatment or receive concomitant medication • Knowledge of treatment could affect decisions as to whether a given subject’s results should be included in analysis
Trial Design Issues • Choice of endpoints • Data to collect • Controls and trial designs/SOC issues • Blinding • ITT analysis/Imputation of missing data • Stratification • Covariates • Concomitant medications
ITT/Imputation of Missing Data • Important to pre-specify how missing data will be handled especially in relatively small trials (LOCF, WOCF etc); other conservative methods of imputation • Use of responder index: respond at any time, respond at last visit, respond at each visit. Use may maintain power and reduce sample size
Stratification • By disease manifestation • By dose of steroid • Other
Covariate Analyses • Anti-DNA at baseline • Number of organs involved or disease activity at baseline • By center • Other- cytokine levels, complement
Concomitant Medications • Need to define allowable medications at baseline • Other medications such as ACE inhibitors • Rescue medication • Do patients stay in trial? • How much is allowed?
Concomitant Medications cont’d • Steroids • Subtle changes in steroid dose could influence outcomes; • Consider a run-in period to standardize steroid dose; • Dose adjustment specified in protocol; • Change in steroid dose (steroid sparing) must be clinically meaningful
Duration of Studies • May depend on claims sought • could a trial for “treats constitutional changes” be 3 months in duration? • Inactive disease: • time to collect adequate number of flares • Active disease • Acute (induction) • weeks to months? • Chronic (maintenance) • months to year(s)? Extension studies vs phase IV studies (need to consider economic costs)
Practical considerations • May be difficult to perform chronic well controlled trial secondary to flares, changing medications, dropouts, changes in medical practice • In disease that waxes and wanes, short trials may not provide adequate demonstration of efficacy, safety, and durability
Extension Studies • Need to demonstrate maintenance of effect (durability) and safety • Comparator(s): are they needed? • Blinded or open label? • Phase IV commitments • how long? Depends on what needs to be demonstrated
Safety Database • ICH: 300-600 patients for 6 months and 100 for one year (for chronic non-life threatening disorders) • What is standard for a disorder as varied as lupus in which some manifestations are chronic and others acute and life-threatening?
One Size Fits All? • No • Multiple possibilities for “wins”
Factors to Consider in SLE Trial Design • Organ specific vs non-organ specific • Active vs inactive disease • Activity measure vs flare vs other • Superiority vs equivalence • Induction vs maintenance • Short term and long term safety • Data to collect
Acknowledgements • Lee Simon • Jeff Siegel • Douglas Throckmorton • James Witter • Lourdes Villalba • Tatiana Oussova • Carolyn Yancey • Members of DAAODP