Download
1 / 33
330 likes | 541 Views
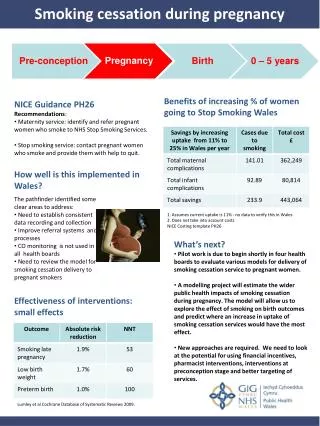
Community Plan Of Care Mecosta County Smoking During Pregnancy. Presented by: Marjanna Barnes Wendy Debruyn Nathan Dixon Elizabeth Klynstra Beth Langenburg Lisa Snider. Introduction.

E N D
Community Plan Of Care Mecosta County Smoking During Pregnancy Presented by: Marjanna Barnes Wendy Debruyn Nathan Dixon Elizabeth Klynstra Beth Langenburg Lisa Snider
Introduction The purpose of this assignment is to identify a problem within a community, analyze the data, provide interventions, provide realistic goals and outcomes, and an evaluation of the plan. Our problem is smoking while pregnant in Mecosta County. Mecosta County has a higher than average poverty rate, less people enrolled in health care services due to cost or no insurance, and have a higher percent of women who smoke while pregnant than the Michigan average. Community based interventions and goals are provided in this presentation.
Assessment of Community Population of Mecosta County • Person’s under 5 years: 22.50% • Person’s under 18 years: 19.80% • Person’s 65 years and over: 16.10% • Median Age of 32 years (District Health Department #10 [DHD], 2014)
Poverty Indicators Mecosta County and State of MI (DHD, 2014)
Access to Health Care Mecosta County and State of MI (DHD, 2014)
Birth Related Statistics Mecosta County and State of MI (DHD, 2014)
2012 and 2013 Chartbook Comparison 2012 Mecosta Michigan Infant Mortality Rate 9.1 7.3 Smoking 25.4% 20.3% Smoking During Pregnancy 31.4% 19.3% Persons Below Poverty 23.6% 15.7% Heart Disease (Cause of Death) 164.2 107.8 District 10 Health Department (2013) 2013 Mecosta Michigan Infant Mortality Rate 7.0 7.1 Smoking 25.4% 20.3% Smoking During Pregnancy 31.6% 19.5% Persons Below Poverty 22.9% 16.3% Heart Disease (Cause of Death) 209.6 201.6 District 10 Health Department (2014) Please note decisions were made for this project based on 2012 chartbook data. Since the start more recent updated information has become available and will be used throughout this presentation. This is just to show original data and compare the differences. (DHD, 2013 & 2014)
Community Health Needs Assessment Positive Indicators • Jobless rate below state rate • Less individuals without a health care provider • Low Birth Weight rate below state and HP2020 • Teen pregnancy rate below state rate (DHD, 2014)
Community Health Needs Assessment Negative Indicators • Persons below poverty threshold greater than state rate • Infant mortality rate greater than state and HP2020 • Greater percentage of uninsured individuals • Greater percentage of individuals that smoke • Greater percentage of smoking during pregnancy (DHD, 2014)
Community Diagnosis Risk of premature birth among pregnant women related to tobacco abuse as demonstrated in the data collected by the District Health Department #10 report for tobacco use during pregnancy in Mecosta county women. (DHD, 2013)
Interventions Already in Place • Six week program at home or in the office (Individual). • Teach effects of smoking on mom and baby, how to break the chain of addiction, and coping skills to stay nonsmoking. • Refer to Michigan tobacco quitline 1-800-quit-now. • Offer program “smoke free baby and me” that uses the five A’s: Ask, Advise to quit, Assess willingness to quit, Assist with quitting, and Arrange follow up. (DHD #10, 2013) (Darcy RN, Personal Communication, April 16, 2014)
Interventions • Include all women of childbearing age in the tobacco use screening.The majority of women who continue to smoke during pregnancy are younger women who are pregnant with their first child (Tong, England, Dietz, & Asare, 2008). • Use the same reliable screening tool at every facility for each individual. Screening is one of the most effective tools for determining individuals at risk for adverse health (Harkness & DeMarco, 2012).
Interventions • Provide education on the seriousness of health risks of smoking to all women of childbearing age. Individuals with a higher education level and higher perceived risk of cigarette smoking are less likely to smoke (Harkness & DeMarco, 2012). • Involve the pregnant mother’s significant other, family, or other support individuals in the education process and together create a plan to quit smoking.Having a support person in the mother’s own social network can be more effective in helping her to quit (Hennrikus, Hellerstedt, Lando, Steele, & Dunn, 2010).
Interventions • Establish a community support group for mothers who are trying to quit smoking.Research shows that pregnant women who have a stronger social capital are better able to control unhealthy behaviors, and improve positive behaviors, like cessation of smoking (Shoff & Yang, 2012). • Provide education and resources for methods of stress reduction that woman can use to replace tobacco use.Maternal stress is related to unsuccessful smoking cessation (Hauge, Torgersen, & Vollrath, 2012).
Interventions • Ensure that all OB GYN offices in the community not only screen for and educate women of childbearing age on the risks of tobacco use at the first visit, but continue to provide ongoing counseling for smoking cessation.Continuing support for smoking cessation is more effective in helping maternal smokers quit (Tong, England, Dietz, & Asare, 2008). • Provide all OB GYN offices in the community with the Maternal Infant Health Program handout from Medicaid and encourage the distribution of the handout to all expectant mothers who qualify (http://www.michigan.gov/documents/mdch/MIHP_Beneficiaries_Brochure-DCH-1416_393191_7.pdf).
Adequacy of Interventions The interventions done by District Health Department # 10 are adequate with the exception of the need for a support group. The reason for the continued problem according to the Maternal and Infant health nurse for Mecosta county is “No OBs will prescribe nicotine replacement therapy.” Most of the interventions are based on the use of nicotine replacement therapy, such as nicotine patches which medicaid will pay for if the Dr. will write a prescription. The Nurse went on to say “We have moms that want to quit but have to do so cold turkey and that is not good for the mom or the baby because of the stress of withdrawal. The OBGYNs in Mecosta county need to be educated on the health effects of smoking versus using a nicotine replacement therapy. Cigarettes are full of so many more chemicals than just nicotine, yet nicotine replacement is not prescribed. The district health department has tried over and over to educate these physicians. (Darcy RN, Personal Communication, April 16, 2014)
Nicotine Replacement During Pregnancy It is thought that nicotine replacement therapy (NRT) is safer than smoking cigarettes while pregnant. Cigarettes contain about 4000 different chemicals and NRT is just nicotine (Osadchy, Kazmin, and Koren, 2009). One study found that there was a three fold increase in quit rates with NRT and behavioral therapy than with behavioral therapy alone (Pollak et al, 2007). It is better to use NRT early in pregnancy than later because there is an increase in nicotine metabolism in the third trimester of pregnancy, therefore more nicotine would be needed (Osadchy, Kazmin, and Koren, 2009). It is best to try to quit without NRT but if she is unable to quit without medication then she should be offered NRT to help quit. It is thought that with NRT there will be increased cessation rates and the fetus will not be exposed to nicotine through the entire pregnancy. NRT is thought to be safer than continuing smoking during pregnancy (www.quit.org).
Change Model • Kurt Lewin’s model of the change process. • A three-stage model of change known as the unfreezing-change-refreeze model. (Chitty & Black, 2011)
Unfreezing Presentation of the problem to gain recognition on the need for change and seeking new solutions. Application Educate on the risk of smoking during pregnancy. Engage physician offices to provide education and prescribe nicotine replacement. (Chitty & Black, 2011)
Transition Development of new behaviors, values and attitudes through process changes and developmental techniques. Application Provide stress reduction techniques to replace tobacco use and engage support system to assist in developing a smoking cessation plan. (Chitty & Black, 2011)
Refreeze Adaption to the new change and sustaining the change over time (Smoking Cessation). Application Encourage participation in community support group to control relapse and reinforce new patterns. (Chitty & Black, 2011)
Policy Implications Positive Public Policy Smoking Cessation Initiatives • Tobacco Tax: Evidence shows that increases in tobacco tax encourage smokers to quit. • Smokefree Laws: Protects nonsmokers from secondhand smoke and encourage smokers to quit by making smoking more difficult. • Over half of the states have passed smoke free laws. • Nurse-Family Partnership: Provides home visits to first-time low-income mothers beginning in pregnancy aiming to promote healthy behaviors (only available in 29 states to date). • Regulation of tobacco products and marketing of products (McGoldrick & Boonn, 2010)
Policy Implications Identified Policy Needs • Public Health Plan coverage of evidence-based smoking-cessation interventions & medications: An estimated 15% of current adult smokers have Medicaid or Medicare but only six state Medicaid programs cover all interventions and medications for smoking cessation. • Information Quitlines: Provide education services and motivation. • Provision of Nicotine Replacement Therapy: Information quitline and provision of nicotine replacement therapy led to a 14.4% decline in smoking in New York City. (McGoldrick & Boonn, 2010)
Goals • Achieve and maintain an average of 19.3% smoking rate in pregnancy by performing education to pregnant women at their initial OB GYN visit by the next District Health Department #10 health report for 2014. • Generate and dispense educational materials to pregnant women with tobacco abuse, resources are at no cost to the recipients, deliver reading to hand out to Mecosta County OB GYN patients. • Create our 2014 strategic plan of reducing smoking among pregnant women in Mecosta County, obtain necessary materials to support success, get approval and agreement to work with OB GYN office in Mecosta County, have action plan in place for start of education and distribution of materials beginning at the initial office visit.
Goal Evaluation Have monthly meetings to evaluate the progress of the smoking cessation in the pregnant women program in Mecosta County, gather feedback from the OB GYN office staff to see what is working and if there is anything that needs to be enhanced. Maintain a log of the progress whether it is positive or negative, have revisions or expansions implemented within a week of the meeting. Continue to examine results until desired percentage rate of below 19.3% of women in Mecosta County smoking while pregnant is achieved.
Goal Evaluation Initiating the tobacco assessment and smoking cessation education to the local OB GYN practices in Mecosta County can be accomplished by making certain that the resources needed to be triumphant in reducing smoking among pregnant women are readily available to hand out upon completion of the smoking assessment at the very first office visit. Having free brochures and other resources available are crucial to reducing the percent of pregnant women smoking in Mecosta County. The smoking rate in pregnancy will be reassessed each year by the District #10 Health Department as part of the annual health report. If data shows that the smoking cessation efforts are not on the decline then reevaluation of the program process would need to be performed.
Evaluation of effectiveness • Outcome desired is lower rate of pregnant mothers in Mecosta county who smoke. Effectiveness would be determined by the 2014 District Health Department #10 health report for Mecosta county indicating 19.3% or less of pregnant mothers who smoke. This outcome may take more than the desired one year time period due to its aggressive nature. • Outcome desired is educational material provided to and accepted by pregnant mothers from local OB GYN providers. Effectiveness would be determined by follow up calls or visits to OB GYN offices, and pregnant mothers who utilized services from those offices, to verify the educational material was distributed and received.
Conclusion Compared to Michigan statistics, Mecosta County has a higher than average percentage of women who smoke while pregnant. Although birth related statistics in the areas of low birth weight and infant mortality are somewhat favorable in Mecosta County compared to Michigan statistics, the risk of infant morbidity and mortality is significantly increased with smoking. Community based interventions are necessary to decrease the incidence of smoking while pregnant and defined goals are required to evaluate the effectiveness of the interventions. To achieve change with smoking behavior in pregnant women, ongoing education and support is necessary by all members of the health care team.
References Chitty, K. K.,& Black, B. P. (2011). Professional nursing: Concepts and Challenges (6th ed.). Maryland Heights, MO: Saunders District Health Department #10 [DHD]. (2014). Health profile chartbook 2013: Mecosta County. Retrieved fromhttp://dhd10.org/images/Mecosta_Chartbook_2013__Feb_18_2014.pdf District Health Department #10 [DHD]. (2013). Health profile chartbook 2012: Mecosta County. Retrieved fromhttp://dhd10.org/images/Mecosta_Chartbook_2012_April_2_2013.pdf Harkness, G.A. & DeMarco, R.F., (2012). Community and public health nursing: Evidence for practice. Philadelphia, PA: Lippincott Williams & Wilkins Hauge, L.J., Torgersen, L, Vollrath, M. (2012). Associations between maternal stress and smoking: findings from a population-based prospective cohort study. Addiction, 107(6), 1168-1173. doi: 10.1111/j.1360-0443.2011.03773.x
References Hennrikus, D., Pirie, P., Hellerstedt, W., Lando, H.A., Steele, J. & Dunn, C. (2010). Increasing support for smoking cessation during pregnancy and postpartum: Results of a randomized controlled pilot study. Preventive Medicine, 50(3), 134-137. doi: 10.1016/j.ypmed.2010.01.001 McGoldrick, D. & Boonn, A. (2010). Public policy to maximize tobacco cessation. American Journal of Preventive Medicine, 38(3), 327-332. Muecke, M. A. (1984). Community health diagnosis in nursing. Public Health Nursing, 1(1), 23-35. Osadchy, A., Kazmin, A., & Koren, G. (2009). Nicotine Replacement Therapy During Pregnancy: Recommended or Not Recommended? Journal of Obstetrics and Gynaecology Canada, Aug(2009), 744-747.
References People, H., & US Department of Health and Human Services. (2011). Healthy People 2020. Pollak KI, Oncken CA, Lipkus IM, Lyna P, Swamy GK, Pletsch PK, et al. (2007) Nicotine replacement and behavioral therapy for smoking cessation in pregnancy. American Journal of Preventive Medicine, 33(4), 297-305. Shoff, C. & Yang, T (2012). Understanding maternal smoking during pregnancy: Does residential context matter? Social Science & Medicine, 78, 50-60\ Tong, V.T., England, L.J., Dietz, P.M., Asare, L.A. (2008). Smoking patterns and use of cessation interventions during pregnancy. American Journal of Preventive Medicine, 35(4), 327-333. www.quit.org (2014) Can I Use Nicotine Replacement Products or Quitting Medications During Pregnancy? Retrieved from: http://www.quit.org.au/about/frequently-asked-questions/faqs-pregnancy-and-quitting-smoking/faq-pregnancy-quitting-medications.html