Download
1 / 25
430 likes | 1.2k Views
Glucocorticoids. Dr. Alia Shatanawi 24-2-2013. Introduction. Adrenal gland: Cortex and Medulla Adrenal cortex: 3-layer Outer: zona glomerulosa: Middle: zona fasciculata Inner: zona reticularis. Corticosteriods Mineralocorticosteriods (Aldosterone)

E N D
Glucocorticoids Dr. Alia Shatanawi 24-2-2013
Introduction • Adrenal gland: Cortex and Medulla • Adrenal cortex: 3-layer Outer: zona glomerulosa: Middle: zona fasciculata Inner: zona reticularis
Corticosteriods • Mineralocorticosteriods (Aldosterone) • Glucocorticosteriods (Glucocorticoids) • Androgens and estrogens
Hypothalamic-pituitary-adrenal axis - HYPOTHALAMUS CRF - - ANTERIOR PITUITARY ACTH METYRAPONE - ADRENAL CORTEX GLUCOCORTICOIDS MINERALOCORTICOIDS
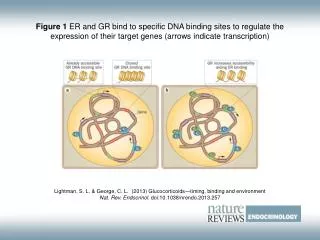
Glucocorticoid Receptors • Members of nuclear receptor superfamily. • nuclear receptors are a class of proteins found within cells that are responsible for sensing steroid and thyroid hormones and certain other molecules. In response, these receptors work with other proteins to regulate the expression of specific genes, thereby controlling the development, homeostasis, and metabolism of the organism • Two GR isoforms: hGRα and hGRβ. • Regulate 10-20% of all genes. • GR: Also present in hypothalamas and anterior pituitary. • Cortisol: equal affinity for MR and GR. • 11-β-hydroxysteroid dehydrogenase converts cortisol to cortisone (minimal MR affinity). • Additional non-genomic effects.
Glucocorticoids • Affect carbohydrate and protein metabolism • Anti-inflammatory and immunosupressive activities • main endogenous hormones: hydrocortisone (cortisol), corticosterone • Secreted from zonafasciculata of AG (middle layer) • Average daily excretion of cortisol: 10-20 mg • cortisol half-life 1.5 hrs • Bind to: corticosteroid-binding globulin (CBG) and albumin
Physiologic Effects of Glucocorticoids:Carbohydrate, Protein and Lipid Metabolism. • Increase gluconeogenesis. • Increase protein catabolism. • Increase blood glucose, insulin secretion and decrease glucose uptake. • Activate glycogen synthase and increase storage of glucose as glycogen. • Stimulate lipase and increase lipolysis. • Fat redistribution. • Antagonize effects of Vit D on Ca+2 absorption.
Physiologic Effects: Anti-inflammatory and immunosuppressive effects. • Suppress leukocyte concentration, distribution and function. • Suppress cytokines and chemokines. • Inhibit macrophage function. • Reduce PLA2 and COXII activities.
Chronic Primary Adrenocortical Insufficiency(Addison’s Disease) Defficiency in corticosteroid production Symptoms: muscular weakness, low BP, depression, anorexia, loss of weight, hypoglycemia, GI disturbances. Minor noxious stimuli may be fatal. Etiology: autoimmune, destruction of gland by chronic inflammatory conidtions (e.g., TB) or discontinuation of chronic glucocorticoid treatment Treatment: 20-30mg cortisol/day + mineralocorticoid, AM, to mimic circadian rhythm.
Acute Primary Adrenocortical Insufficiency Cause:Waterhouse-Friderichsensyndrome, sudden withdrawal of long-term corticosteroid therapy and stress in patients with underlying chronic adrenal insufficiency Aim of therapy:correct fluid and electrolyte imbalance. Treatment: 100mg cortisol iv q8h until pt stable reduce to maintenance within 5 days. resume mineralocorticoid when cortisol at 50mg/day.
Waterhouse-Friderichsen syndrome Adrenal gland failure due to bleeding into the adrenal glands, caused by severe bacterial infection Most commonly the meningococcusNeisseria meningitidis Massive blood invasion, organ failure, coma, low blood pressure and shock, disseminated intravascular coagulation (DIC) with widespread purpura, rapidly developing adrenocortical insufficiency and death.
Congenital Adrenal Hyperplasia Familial disorder of cortisol synthesis enzyme deficiency Excessive ACTH production Most common due to 21 hydroxylase deficiency. Treatment: Cortisol (12-18 mg/m2/day, po) or alternate day prednisone or predinisolone Fludrocortisone (0.05-0.2 mg/day, po); salt. (moderate glucocorticoid potency and much greater mineralocorticoid potency) Over production of Androgens: virilization, accelerated growth and early epiphysial fusion
Cushing’s Syndrome Excess glucocorticoid production due to bilateral adrenal hyperplasia secondary to pituitary adenoma. Symptoms: euphoria, buffalo hump, moon face, easy bruising, poor wound healing, hypertension, cataracts, thinning of skin, increased abdominal fat, thin arms and legs, muscle wasting,osteoporosis, increased susceptibility to infection, obesity. Treatment: remove or irradiate tumor or resect AG 300mg cortisol iv on surgery day. reduce to replacement levels.
Non-adrenal disorders Anti-Inflammatory – potency related to half-life. Immunosuppression – myasthenia gravis, rheumatoid arthritis, lupus, organ transplantation. Cause lymphatic tissue atrophy and reduce macrophage activity. Allergic disorders - asthma, bee stings, allergic rhinitis, contact dermatitis, hay fever. Cerebral edema – dexamethasone after brain/spinal cord trauma Eye disease - conjuctivitis, choroiditis, optic neuritis. Dexamethasone to reduce inflammation. GI disorders - Inflammatory bowel disease (Crohn’s), sprue, ulcerative colitis.
Non-adrenal disorders Leukemia - lymphocytic leukemia. Neurological - multiple sclerosis. Pulmonary - pneumonia, prevention of IRDS Renal - nephrotic syndrome. Rheumatic carditis - alter function of NE receptors. Septic Shock – Dermatological - eczema, dermatitis (topical steroids). Thyroid - malignant exophthalmos, subacute thyroiditis Collagen - giant cell arteritis, temporal arteritis
Anti-inflammatory and Anti-immunologic Therapy • Steroids are potent drugs for interrupting events triggered at the cell membrane (prostaglandins, phospholipase, etc.), and cell mediated immunity (antigen recognition, cell migration, etc.) • Steroids are NOT effective inhibitors of antibody synthesis. • Dosing To Reduce inflammation • various "protocols" lead to success • Discontinuing therapy • Cold turkey if glucocorticoid therapy of less than 2 weeks duration • Taper off if Glucocorticoid therapy of greater than 2 weeks duration. • Rate of taper should be proportional to duration of prior therapy. • The longer the original therapy, the slower the rate of dose reduction.
Glucocorticoids: unwanted efffects • Cushing’s disease • Conn’s disease • GI: peptic ulcer, fatty liver, pancreatitis, N&V. • Metabolic: hyperglycemia, protein wasting, hyperlipidemia, obesity. • Musculoskeletal: myopathy, growth failure, osteopenia. • Ocular: cataracts, glaucoma. • CNS: insomnia, nervousness, depression, bipolar disorder, schizophrenia. • Endocrine: suppression of HPA axis, increased PTH secretion, antagonism with insulin, PTH, TH.
Primary Aldosteronism(Conn’s Syndrome) Excess mineralocorticoid production due to hyperactivity ortumor of the adrenals. Suppressed levels of PRA and angiotensin II Symptoms: hypertension, weakness Treatment: spironolactone.
Glucocorticoids: unwanted efffects • Fluid & Electrolyte balance: Na+ retention, K+ loss, negative Ca++ balance, glycosuria. • Skin: thinning of the skin, striae, purpura, ecchymoses, acne, hirsuitism. • General: Cushingoid appearance with truncal obesity increased risk for bacterial, fungal, viral infections.
Glucocorticoids inhibit some portions of the immune response, they are used in treatment of a large number of diseasesThe following list includes some of the established uses of systemic corticosteroids.: • acute, severe allergic reactions • arthritis, osteoarthritis, rheumatoid arthritis, psoriatic arthritis, and gouty arthritis • adrenocortical insufficiency • allergic conjunctivitis • allergic rhinitis • anemia • (acquired hemolytic and congenital hypoplastic) • ankylosing spondylitis • asthma • beryliosis • bursitis • corneal ulcers • Crohn'sdisease • dermatitis (atopic, contact, exfoliative, and seborrheic) • dermatomyositis • erythema multiforme • erythroblastopenia • herpes zoster of the eye • hypercalcemia secondary to cancer • hypersensitivity reactions • idiopathic thrombocytopenic purpura • leukemia • lupus erythematosis • lymphoma • multiple myeloma • multiple sclerosis, acute exacerbations • mycosis fungoides • optic neuritis
Cont…. • pemphigus • pneumonitis (aspiration) • rheumatic carditis • Stevens-Johnson syndrome • thrombocytopenia • trichinosis with nerve or heart involvement • tuberculosis, disseminated and fulminating • tuberculous meningitis • ulcerative colitis