Download
1 / 43
500 likes | 1.09k Views
Normal anatomy of the liver. Diaphragmatic surface of the liver is dome-shaped , follows the contours of the diaphragm , reaches forward as far as the inferior edge of the liver. Inferior margin of the liver

E N D
Diaphragmaticsurface of theliver isdome-shaped, followsthecontours of thediaphragm, reachesforward as far as theinferioredge of theliver
Inferiormargin of theliver its major landmarkisthesagittalgroove, a deepnotch for theligamentumtereswhichrunsinthefreeedge of thefalciformligament Incisura ligamenti teretis margo inferior Incisura vesicae fellae
Inferiormargin of theliver T2 BLADE
Visceralsurface of theliver Porta hepatis – a central depression for thepassage of the portal vein, hepaticartery and common bile duct Anterior to thisisthegallbladderfossawiththequadratelobe to itsleft Posteriorlythecaudatelobeseparatesthe porta from IVC Severalshallowimpressionsrelate to theshape of adjacentorgans
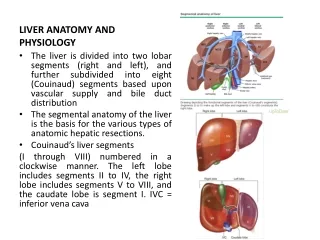
Externallobation of theliver The H-shaped indentations on the visceral faces of the liver divide it into four lobes: the right, left, quadrate and caudate lobes. The right-hand limb of the H is formed by the gallbladder fossa anteriorly and by the IVC sulcus posteriorly The left limb of the H is formed by anteriorly – the deep fissure for the ligamentum teres and posteriorly by the fissure for the ligamentum venosum * **
Segmentalliveranatomy Segmental liver anatomy. The segmental anatomy of the liver as described by Couinaudand Bismuth. Each anatomic segment receives a unique portal pedicle (dark gray) consisting of a portal venous branch, hepatic arterial inflow, and bile duct. Individual segments are drained by unique hepatic venous outflow branches (light gray) and separated by connective tissue scissurae.
Segmentalliveranatomy Couinaud divided the liver into a functional left and right liver by a main portal scissurae containing the middle hepatic vein. This is known as Cantlie's line. Cantlie's line runs from the middle of the gallbladder fossa anteriorly to the inferior vena cava posteriorly. • Portal vein– superior nad inferiorsegments • Righthepaticvein– anterior and posteriorsegments of RL (5,6,7,8) • Middle hepaticvein– Cantlie’s line • Lefthepaticvein– medial and lateralsegments of LL (4,2,3)
There are eight liver segments.Segment 4 is sometimes divided into segment 4a and 4b according to Bismuth.The numbering of the segments is in a clockwise manner (figure).Segment 1 (caudate lobe) is located posteriorly. It is not visible on a frontal view.
Segmentalliveranatomy - CT 2 7 8 3 4 6 5
Segmentalliveranatomy US 2 8 7 3 4 6 5
Biliarytractanatomy Theright and leftmainhepaticductsfuseatthe hilum, anterior to thebifurcation of the portal vein, to form thecommonhepaticduct. The main bile duct is divided into two segments: the commonhepatic duct and common bile duct, divided by the cystic ductinsertion.
Biliarytractanatomy Thelefthepaticductdrains 3 segmments of theleftliver, and therighthepaticduct 4 segments of therightliver. Therighthepaticductarisesfromthe union of twomainsectorialducts: an anteriordivisiondrainingsegments 5 and 8 and a posteriordivisiondraining 6 and 7. Thecaudatelobe (segment 1) has a variabledrainagepattern, but inthemajority (78%) drainageisintobothmainducts.
Biliarytractanatomy The common bile duct passes inferiorlyposterior to the first part of the duodenum and pancreatichead. In the majority it then forms a short common channel with the main pancreatic duct within the wall of the duodenum, termed the ampulla of Vater.
Biliarytractanatomy Thecommon bile duct lenght - 5-15cm depending on thelevel of thecysticductinsertion diameter - up to 6mm, inelderly 8mm, aftercholecystectomyup to 10mm.
Biliarytractanatomy Gallbladder - a bilereservoir, lies in the cystic fossa Thecysticduct- lenght 2-4cm, diameter 1-5mm, joinsthecommonhepaticductinitssupraduodenal segment, halfthewaybetweentheliver hilum and ampulla of Vater US, CT- visible in 50% of cases MRCP- almost always visible
Biliarytractanatomy MRCP
Developmentalanomalies of biliarytractanatomy Insertion of right posterior sectoral duct into left hepatic duct
Livervascularsupply • portal supply • arterialsupply • venousoutflow
Livervascularsupply Portal supply Theliverreceivesapp. 2/3 of itsbloodsupplyfromthe portal vein. Normallythe superior mesentericvein and splenicveinbecomeconfluent to form a single portal vein, whichcourses to thehepatic hilum and dividesintotherightendleftbranch. Portal veinlenght – 6-7cm, diameter 6-13mm.
Livervascularsupply Venousoutflow – three major hepaticveinsdrainintothe IVC
The collateral vessels in portal hypertension. AWV = abdominal wall vein, GEV = gastroesophageal vein, IMV = inferior mesenteric vein, IVC = inferior vena cava, LGV = left gastric vein, LPV = left portal vein, LRV = left renal vein, MV = mesenteric vein, PDV = pancreaticoduodenal vein, PEV = paraesophageal vein, PV = portal vein, RPPV = retroperitoneal-paravertebral vein, SMV = superior mesenteric vein, SRV = splenorenal vein, SV = splenic vein, UV = umbilical vein.
Livervascularsupply Arterialsupply– hepaticarteryproper – 20% of bloodsupply Theusualarterialarrangementis for thecommonhepaticartery to arise as one of thethree major branches of thecoeliactrunk. Aftergivingoffthegastroduodenalartery , itcontinues as themainhepaticartery, whichinturnsdividesintotheright and lefthepaticarteries.
Livervascularsupply Hepaticarteryproper
Normal Anatomy of the Pancreas The pancreas is a retroperitoneal organ and is positioned in the anterior pararenal space. It is posterior to the stomach and lesser sac and anterior to the abdominal aorta and upper lumbar vertebrae.
Normal Anatomy of the Pancreas CT Parenchymal phase The normal pancreatic parenchyma has CT attenuation values in the range of 30-60 HU. Pancreatic attenuation decreases due to fatty infiltration which occurs normally with aging.
Normal Anatomy of the Pancreas 1- liver 2- head of the pancreas 3- pancreatic body 4- Wirsung's duct 5- tail of the pancreas 6- superior mesenteric artery 7- vena cava inferior 8- aorta 9- spine 10- gallbladder neck The normal pancreas is of similar echogenicity to theliver.
Normal Anatomy of the Pancreas Normal pancreatic duct
Normal Anatomy of the Pancreas MRCP Normal MRCP performed during secretin stimulation shows a slight and temporary increase in the caliber and signal intensity of the main pancreatic duct in A (arrow) andprogressive and complete duodenal filling (arrowheads in B). Complete filling of the Santorini duct (arrowhead in A) is also seen.
Normal Retroperitoneal Anatomy Anterior Renal Fascia Posterior Renal Fascia
Anterior Pararenal Space • Boundaries • Anteriorly: post parietal peritoneum • Posteriorly: ARF • Contents: Ascending and descending colon, duodenum, pancreas • Continuous across midline, with root of small bowel mesentery and inferiorly with perirenal, posterior pararenal and prevesical spaces
Posterior Pararenal Space • Boundaries • Anteriorly: PRF and lateral conal fascia • Posteriorly: transverse fascia • Limited by and parallels psoas m. • Open laterally to flank and inferiorally to pelvis • Contents: Fat (no visceral organs) • Continuous (potentially) with each other via properitoneal fat of anterior abdominal wall
Interfascial Retroperitoneal Planes • Retromesenteric - between anterior pararenal and perinephric spaces contiguous across midline and laterally with retrorenal and lateral conal space • Retrorenal - between perinephric and posterior pararenal spaces • Lateral conal • * Combined fascial plane continues into pelvisanterolateral to psoas m. allowing pathway to pelvis • * Trifurcation of 3 planes - anterioposterior location isvariable
The Perirenal Space • Anterior and post renal fasciae • Extent: Superior, medial, lateral, inferior • Contents
Extent of Perirenal Space • Superior - open to bare area of liver and contiguous with mediastinum • Medial - above renal hila perirenal spaces are separate, beginning at level of hila there is communication • Lateral - ARF, PRF fuse to form lateral conal fascia • Inferior - ARF & PRF converge blend about 8 cm below kidney
Contents of Perirenal Space • Kidney, proximal collecting system, renal septa, adrenal gland • Renal vasculature and perirenal vessels • Lymphatics • Bridging septa