Download
1 / 38
380 likes | 395 Views
Common Opportunistic Infections in HIV Patients, Part 2. Chris Farnitano, MD Thursday, October 8, 2009 Noon Conference. Objectives. Discuss most common opportunistic infections (OIs): Dx and Rx Discuss immune reconstitution disease Review primary OI prophylaxis. Forms. Case Study SP.

E N D
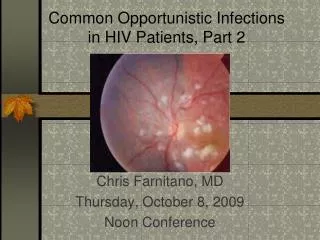
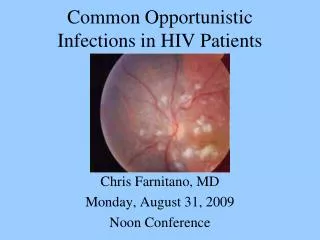
Common Opportunistic Infections in HIV Patients, Part 2 Chris Farnitano, MD Thursday, October 8, 2009 Noon Conference
Objectives • Discuss most common opportunistic infections (OIs): Dx and Rx • Discuss immune reconstitution disease • Review primary OI prophylaxis
Case Study SP • 27 yo male seen in clinic in June 2009 • Meds: unboosted atazanavir + Truvada since 1/09; ranitidine • T cells 5; viral load 30,000 • Why is his anti-HIV cocktail failing?
Case Study SP • Ritonavir added to boost atazanavir • Patient instructed to take ranitidine in AM only and antivirals in PM • Blood Cx for AFB, HIV genotype ordered
Case Study SP • Admitted to Kaiser August, 2009 with diffuse warm, tender lymphadenopathy • Biopsy performed, read as suspicious for lymphoma • Transferred to CCRMC after 7 days on clarithromycin, ethambutol, rifabutin • T Cells 209, viral load 726 • What is patient’s diagnosis?
What are the most common OI’s? • Cohort Studies in pre-triple therapy era: • Candida • Pneumocystis Carinii • Cytomegalovirus • Mycobacterium Avium Complex • Pneumocystis - second episode • Toxoplasmi gondii • Herpes zoster
Causes of death, PHC HIV clinic • 2007-9 • RH: Crypto meningitis • TW: street drug overdose • SA: sepsis, pneumonia and massive hemoptysis • DW: metastatic prostate ca • RP: CVA, laryngeal ca • VA: PML (progressive multifocal leukencephalopathy) • AM: bacterial pneumonia, ETOH cirrhosis, wasting
OIs diagnosed, PHC HIV clinic • 2005-9 • PCP pneumonia • Esophageal Candidiasis • Herpes Simplex • Herpes Zoster • M. Kansasii immune reconstitution pneumonia • Mycobacterium Avium Complex (MAC) • Cryptococcal Fungemia, meningitis • Histoplasmosis • PML
Effect of HAART on Opportunistic Infection Incidence • Most OI’s have declined 80-90% • OI’s seen now mostly in 3 groups • undiagnosed HIV+ • not in care or not adhering to therapy • long time “battle-scarred warriors” failing after a long history of multiple regimens
50-200 T Cells: • Pneumocystis Carinii Pnuemonia • Toxoplasmosis • Cryptococcus
<50 T Cells • CMV Retinitis • Mycobacterium Avium Complex • Cryptosporidiosis • Progressive Multifocal Leukencephalopathy
Ockham's razor does not apply for advanced AIDS • -often multiple diagnoses present simultaneously • ie PCP, CMV, KS, Cocci • 12% of bacterial pneumonias also have PCP • 10% of PCP pneumonia complicated by bacterial infection • search for second etiology if patient not improving
Immune reconstitution diseases(HAART attacks) • MAC adenitis • CMV • TB • PCP
Case Study SP • Diagnosis: Immune Reconsitution MAC • AFB blood culture from June grew out MAC on 8/12 (hospital day #13) • Also: • Perianal herpes • Squamous cell carcinoma-in-situ, buttock • Vancomycin-resistant enterococcus, groin
Primary OI prophylaxis • PCP -T cells <200 or thrush • Toxo -T cells <100 and +Toxo titer • MAC - Tcells <50 • TB – INH x 9 months if PPD >5mm or quantiferon-TB positive
Toxo prophylaxis • Septra SS or DS qd or DS TIW • Septra Desensitisation: • 1cc qd x 3d, then 2cc qd x 3d, then 5ccqd x 3d, then one SS tab qd • Dapsone 100mg qd +pyramethamine 50mg qweek + leukovorin 25mg qweek • Atovaquone 1500mg qd
MAC prophylaxis • Zithromax 600mg x 2 tabs qweek reduces infection rate 59% • Also seems to reduce risk of PCP
Cytomegalovirus Retinitis - Who Gets It? • Rare above 50 T Cells • Reactivation disease: most HIV patients CMV IgG+ (90% of gay HIV+ men) • 90% of CMV disease is retinitis
Cytomegalovirus Retinitis - Symptoms • painless, progressive visual loss • unilateral blurry vision • floaters
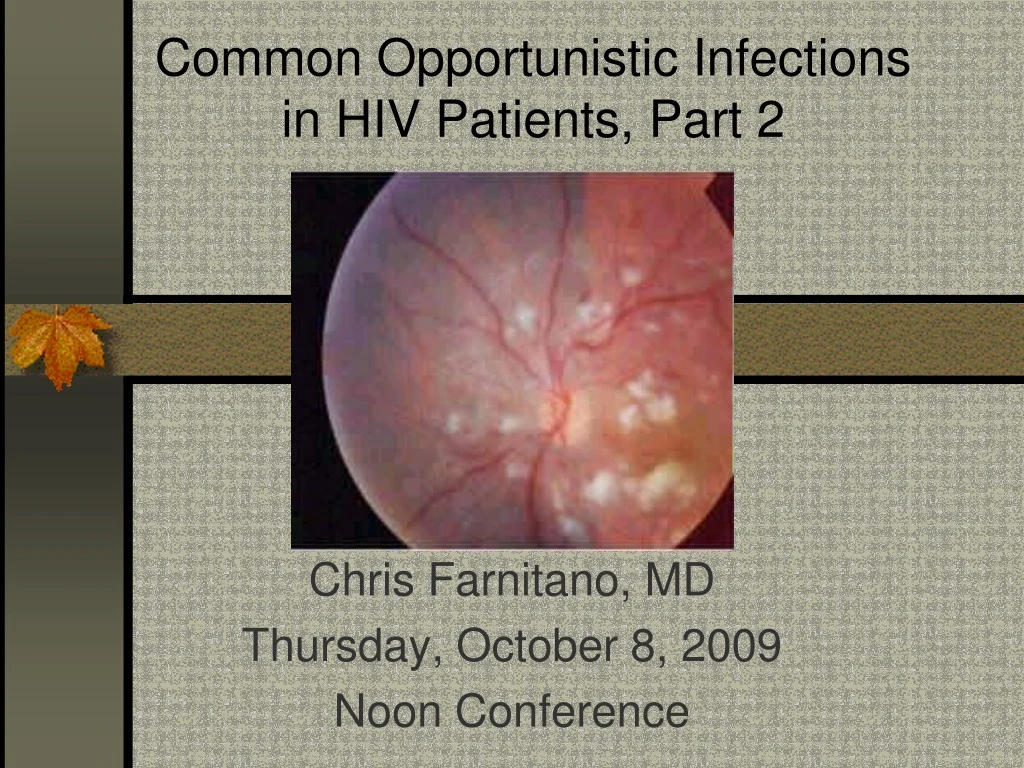
Cytomegalovirus Retinitis - Signs • coalescing white perivascular exudates • surrounded by hemorrhage • brushfire pattern or tomato and cheese pizza
Cytomegalovirus Retinitis - Diagnosis • if you suspect it, obtain ophthalmologist confirmation within 24-48 hrs.
Cytomegalovirus Retinitis - Treatment • Valgancyclovir 900mg PO BID x 21 days, then qd • Adverse effects: • neutropenia ANC<500 in 15% • thrombocytopenia • anemia • 50%: nausea, vomiting, abdominal pain or diarrhea
Gangcyclivir intraocular implant • Consider in addition to systemic therapy: • Surgically implanted depo device • Effective for 6 months • Replace at 6 months if still not immune reconstituted • Consider for sight threatening lesions near the central visual field
Mycobacterium avium Complex - Who gets it? • T Cells <50 • screen with blood culture for AFB x 1 q 3 months to detect subclinical disease
Mycobacterium avium Complex - Symptoms • fever, night sweats • weight loss • diarrhea
Mycobacterium avium Complex - Signs • anemia • Neutropenia • Fever • Diarrhea • wasting
Mycobacterium avium Complex - Diagnosis • Blood culture usually positive if symptomatic but takes weeks to grow • If need to know sooner then do bone marrow Bx • Positive sputum culture usually colonization, not active disease • Positive stool culture may be colonization, not active disease, mucosal bx more indicative of disease
Mycobacterium avium Complex - Treatment • Clarithromycin 500mg BID + • Ethambutol 15mg/kg/d +/- • Rifabutin 300mg qd • Treatment failure rate is high without immune reconstitution • drug toxicity • development of resistance
Case Study SP • After 4 months of anti-MAC therapy + potent anti-HIV therapy: • T Cells 71 viral load <48 • Patient still hospitalized • Large effusions persist • Dubhoff tube required for feeding • Diffuse chest/abdominal adenopathy persists • MAC Cx’s show partial/complete resistance to all MAC drugs except clofazamine • Prognosis?
Summary: • Pyramid approach • Prophylaxis simple: Septra and Zithromax • Rule out TB in pneumonia with T Cells <200 • Avoid treating PCP empirically • An ounce of prevention pills is worth a pound of Treatment pills
An ounce of prevention pills is worth a pound of Treatment pills