Download
1 / 34
350 likes | 527 Views
New directions in advanced kidney cancer: the ARISER and VEG102616 studies. Jonathan Rosenberg, MD UCSF Cancer Center Survivor’s Day 2006. Agenda. Staging for kidney cancer Adjuvant therapy trial: ARISER Advanced kidney cancer trial: Pazopanib (GW786034).

E N D
New directions in advanced kidney cancer: the ARISER and VEG102616 studies Jonathan Rosenberg, MD UCSF Cancer Center Survivor’s Day 2006
Agenda • Staging for kidney cancer • Adjuvant therapy trial: ARISER • Advanced kidney cancer trial: Pazopanib (GW786034)
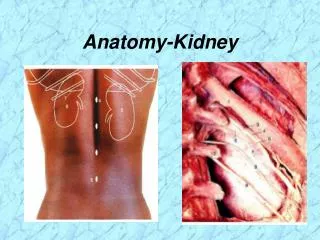
Clinical Staging and Prognosis in RCC: American Joint Committee on Cancer Criteria Stage I Tumor <7 cm in greatest dimension andlimited to kidney; 5-year survival, ~95% Gerota’s fascia Adrenal gland Aorta Kidney Stage II Tumor >7 cm in greatest dimension andlimited to kidney; 5-year survival, ~88% Inferior vena cava Stage III Tumor in major veins or adrenal gland,tumor within Gerota’s fascia, or 1 regional lymph node involved;5-year survival, ~59% Lymph nodes Stage IV Tumor beyond Gerota’s fascia or>1 regional lymph node involved;5-year survival, ~20% Modified from Cohen HT, McGovern FJ. N Engl J Med. 2005;353:2477-2490.
Clinical Staging and Prognosis in RCC: AJCC System Javidian J et al. J Urol 1999;162:1277-1281.
Surgical Management of RCC • Surgery is the primary approach for early-stage (T1–T2), localized kidney cancer • Partial vs radical nephrectomy • Laparoscopic vs open surgery • RFA or cryotherapy are sometimes considered • Surgical removal of locally advanced RCC (T3) is associated with high recurrence • 20%–30% of patients with localized tumors recur, usually within 3 years • Systemic therapy has not been proven to be effective in reducingrisk of relapse • Surveillance (X-ray and CT) is recommended for all patients and should be more frequent for patients with higher stage tumors • Patients should be considered for clinical trial enrollment testing strategies to prevent recurrence
Limited Role of Adjuvant Therapy inRCC BCG=Bacillus Calmette-Guerin; DFS=disease-free survival; IFN-=interferon alpha; IL-2=interleuken 2; MPA=medroxyprogesterone acetate; NS=not significant; PFS=progression-free survival. 1. Jocham D et al. Lancet. 2004;363:597-599;2. Kjaer M et al. Int J Radiat Oncol Biol Phys. 1987;13:665-672; 3. Pizzocaro G et al. J Urol. 1987;138:1379-1381; 4. Galligioni E et al. Cancer. 1996;77:2560-2566; 5. Messing EM et al. J Clin Oncol. 2003;21:1214-1222; 6. Clark JI et al. J Clin Oncol. 2003;21:3133-3140.
Advanced kidney Cancer • Curing kidney cancer once it recurs is very difficult • Prevention of recurrence in patients who have their kidneys removed is a “holy grail” of kidney cancer • “Adjuvant therapy” • Treatment given after the main therapeutic intervention to reduce the risk of recurrence • No therapy yet has proven beneficial in reducing recurrence • Effective new treatments are needed
Rencarex: Wilex G250 antibody • High affinity chimeric antibody • Targets the MN/ carbonic anhydrase IX (CAIX) antigen • 95% of clear cell kidney cancer express this antigen • CAIX not expressed in normal kidney and in other tissues • How does it work? • G250 binds to kidney cancer cells and targets them for destruction by the immune system • “Antibody dependent cell-mediated cytotoxicity”
Rencarex: Wilex G250 antibody • Initially tested in metastatic kidney cancer • Low response rate in metastatic kidney cancer but high rate of stable disease • Patients with clinical benefit (response or stable disease) did better than those who did not • Excellent safety profile • No serious side effects observed • Low toxicity and results from the early testing provide rationale for testing it to prevent or delay recurrence
G250 Adjuvant Study:ARISER Adjuvant Rencarex (WX-G250) Immunotherapy Phase III trial to Study Efficacy in Non-metastatic Renal Cell Carcinoma • Randomized • Double blind • Placebo controlled • Clear cell kidney cancer with high risk of recurrence
ARISER G250 Study • Who can enroll: • T3bN0/NX (into the renal veins or vena cava below the diaphragm) • T3cN0/Nx (into the vena cava above the diaphragm or into the wall of the vena cava) • T4N0/NX (outside the kidney fascia) • Any T stage and Node + • T1bN0/NX (tumor between 4 and 7 cm) or T2N0 (>7cm but limited to the kidney) with microscopic vascular invasion • T3aN0/NX (invades adrenal gland or peri-renal fat) and grade 3 or higher
ARISER G250 Study • Other major eligibility criteria: • No history of prior cancer, immunotherapy, chemotherapy within 5 years • No immunosuppression or corticosteroid therapy • When can they enroll: • Within 8 weeks of nephrectomy
Nephrectomy Screen Randomize G250 antibody infusion weekly x 6 months Placebo infusion weekly x 6 months CT Chest, Abdomen, Pelvis monitoring Follow for 6 years Study Design 612 patients needed Study is designed to answer the question of whether this treatment will be effective in preventing recurrence and improving survival
Advanced kidney cancer • RCC highly resistant to current chemotherapy drugs • Interferon- • 15% objective response rate (ORR) • responses rarely complete or durable • modest survival benefit compared with placebo or ineffective therapies • High-dose interleukin-2 • 15-20% ORR in stage IV patients • only 5% complete responders • No overall benefit to high dose IL-2 compared to low dose therapy • 3-5% of patients have durable responses
VEGF-targeted tyrosine kinase inhibitors (TKI’s) • Approval of 2 new drugs for kidney cancer (sorafenib, sunitinib) represents a major advance • Need to identify the best anti-VEGF tyrosine kinase inhibitor for patients with advanced kidney cancer • The “best” drug has not yet been defined • Goals of current kidney cancer research is to give patients more and better options • Testing of new drugs in this class may find different levels of anti-cancer activity and side effects
What is Pazaponib (GW786034)? • Pazopanib (GW786034) is a potent multi-target tyrosine kinase inhibitor that inhibits VEGFR-1, -2. -3, PDGFR- and -, and c-kit • Selectively inhibits VEGF-mediated endothelial cell proliferation • Once daily dosing of tablets (800mg) • Pazaponib has been given to 200+ patients
Pazopanib (GW786034) Development • The first study (VEG10003) in various advanced solid tumors : • Phase I • Dosed subjects at various levels (50mg to 2000mg) to find the appropriate dose for the oncology program • The appropriate dose turned out to be 800mg • Many other studies in other cancer types being conducted with this drug
Pazopanib (GW786034) Development in RCC • The Phase I study demonstrated activity (stable disease or partial response) in kidney cancer Baseline Post Treatment (Week 21)
VEG10003 Phase I Patient Background • Enrolled • 63 subjects • 2 cohorts (800mg daily or 300 – 400 mg twice daily) • Tumor types enrolled • Kidney - Renal (12 pts) • Colorectal Cancer - CRC (10 pts) • Sarcoma – soft tissue tumors (8 pts) • Lung (7 pts) • Breast (5 pts) • Pancreatic (4 pts) • GIST - Gastrointestinal stromal tumor (4 pts) • Neuroendocrine (3 pts) • Other (10 pts)
Pazaponib (GW786034) Response in Phase I Several VEG10003 study patients had stable disease or partial responses: - kidney cancer - thyroid cancer (on study for 101weeks or ~2 years) - sarcoma - GIST (gastrointestinal) - ovarian cancer - melanoma (skin cancer) - rectal cancer - lung cancer - neuroendrocrine
Pazaponib (GW786034) Response in Phase I VEG10003 study patients with Kidney cancer: • 7 patients in first study who received 800 mg to 2000 mg daily or 300 mg bid had stable disease or tumor reduction • 3 subjects are still on study: • One with a partial response (PR) • Two with stable disease/minimal response (SD/MR) • 1 subject had a partial response
Pazaponib (GW786034) Side Effects Common side effects seen in at least 2 patients dosed at 800mg for the 11 total subjects include : • Elevated blood pressure (Hypertension) (n=8) • Tiredness (Fatigue) (n=7) • Diarrhea (n=6) • Nausea (n=5) • Protein in urine (Proteinuria) (n=4) • Decrease in neutrophils, a type of white blood cell (Neutropenia) (n=2) • Decreased platelets in the blood (Thrombocytopenia) (n=2) • Vomiting (n=2) • Hair changes color to white (Depigmentation) (n=2)
Comparison of Treatment-emergent Adverse Events * Data from sorafenib and sunitinib label, respectively
VEG102616 Study Details VEG102616: Randomized Discontinuation Study of GW786034 (pazopanib)
VEG102616: New Phase II study • Study is open in 10 countries around the world • 12 sites in the USA • There are several sites in California recruiting for the study:Jonathan Rosenberg, MD UCSF Comprehensive Cancer Center in San Francisco, CA David Minor, MDCalifornia Kidney Cancer Foundation in San Francisco, CAJohn Fruehauf, MDUniversity of California, Irvine in Orange, CA
VEG102616: A Global Study 60+ study sites N = 160-230 patients First patient enrolled: Oct 2005 Europe UK Belgium Czech Republic Israel Asia China Taiwan Hong Kong Malaysia Singapore North America USA Australia
VEG102616 Phase II Trial Design Screening/ Baseline 3 months(open label drug) Lead-in phase Decision point 4 months Randomized drug (stable disease) Open label drug (tumors are smaller) RandomizationPhase *Pts may switch to open label if they progress on randomized drug All subjects Open label drug: continues until indefinitely (unless progression)
VEG102616 Phase II Trial Key Objectives: Lead-in Phase (3 months of study) • To determine the response to drug after the first 3 months of treatment Randomized Phase (4 months of study) • Primary Objective: • Compare the tumor shrinkage of patients on active drug vs. patients on placebo in a randomized setting • Secondary Objectives: • Safety (all patients) • To determine progression-free survival over a 4 month time period in a randomized population • To determine response rate (in terms of tumor shrinkage)
Study entry criteria for Phase II VEG102616? Inclusion: • Clear Cell Kidney Cancer • Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) of 0 or 1. • Adequate bone marrow function. • Adequate kidney function. Exclusion: • Have had any major surgery, radiotherapy, or immunotherapy within the last 28 days and/or not recovered from prior therapy. • Women who are pregnant or lactating. • Poorly controlled hypertension. • Any serious and/or unstable pre-existing medical, psychiatric, or other condition (including lab abnormalities) that could interfere with safety or obtaining informed consent.
VEG102616: Study Procedures Basic study procedures include the following: • Review and consent to the trial (informed consent process) • Review of medical history and medication review • Disease assessment (CT scans, MRI or bone scans) • Blood and urine samples • ECGs (monitor heart) • Physical exams • Vitals and blood pressure monitoring
VEG102616: Contacts for study • Jonathan Rosenberg, MD UCSF Comprehensive Cancer Center San Francisco, CA • David Minor, MDCalifornia Kidney Cancer Foundation San Francisco, CA • GlaxoSmithKline Clinical Trial Center: reference on call study: VEG102616Toll free phone number: 1- 877-379-3718
Summary: GW786034 • Multi-target tyrosine kinase inhibitor of VEGFR, c-Kit and PDGFR • Evidence of anti-tumor activity in advanced RCC and other advanced solid tumors in early programs • Most common side effects • Hypertension • Fatigue • Gastrointestinal • 800 mg once daily is being evaluated in Phase II trials and is the proposed dose for the Phase III trial in RCC
Future directions • Urgent need to improve options for patients to prevent recurrence of their kidney cancer after nephrectomy (ARISER) • Identify the best anti-VEGF agent in advanced kidney cancer • Ultimate goal is to have many more survivors here each year