Download
1 / 21
470 likes | 2.22k Views
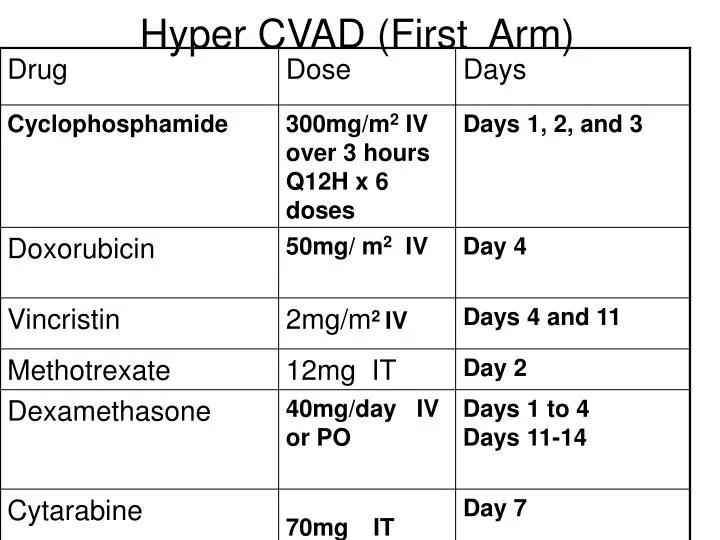
Hyper CVAD (First Arm). MESNA may be given as an uroprotectant at the same total dose as cyclophosphamide but given by continuous infusion starting with cyclophosphamide and ending 6 hours after the last dose. 1)Cyclophosphamide:. Storage

E N D
MESNA may be given as an uroprotectant at the same total dose as cyclophosphamide but given by continuous infusion starting with cyclophosphamide and ending 6 hours after the last dose.
1)Cyclophosphamide: • Storage • Store intact vials of powder at room temperature of 15°C to 30°C (59°F to 86°F). • Reconstituted solutions are stable for 24 hours at room temperature and 6 days under refrigeration 2°C to 8°C (36°F to 46°F). • Further dilutions in D5W or NS are stable for 24 hours at room temperature (25°C) and 6 days at refrigeration • Reconstitution • Reconstitute vials with SWI, NS, or D5W to a concentration of 20 mg/mL. • Compatibility • Stable in D5LR, D5NS, D5W, LR, 1/2NS, NS.
2)Doxorubicin: • Storage • Store intact vials of solution under refrigeration at 2°C to 8°C and protected from light. • Store intact vials of lyophilized powder at room temperature (15°C to 30°C). Reconstituted vials are stable for 7 days at room temperature (25°C) and 15 days under refrigeration (5°C) when protected from light. • Infusions are stable for 48 hours at room temperature (25°C) when protected from light. • Solutions diluted in 50-1000 mL D5W or NS are stable for 48 hours at room temperature (25°C) when protected from light. • Reconstitution • Reconstitute lyophilized powder with NS to a final concentration of 2 mg/mL (may further dilute in 50-1000 mL D5W or NS for infusion). Unstable in solutions with a pH <3 or >7. • Compatibility • Stable in D5W, LR, NS.
3)Vincristin: • Storage • Undiluted vials: Store under refrigeration. May be stable for up to 30 days at room temperature. • I.V. solution: Diluted in 20-50 mL NS or D5W, stable for 7 days under refrigeration, or 2 days at room temperature. In ambulatory pumps, solution is stable for 7-10 days at room temperature. • Reconstitution • Solutions for I.V. infusion may be mixed in NS or D5W. • Compatibility • Stable in D5W, LR, NS.
Methotrxate: • Storage • Store tablets and intact vials at room temperature (15°C to 25°C). Protect from light. • Solution diluted in D5W or NS is stable for 24 hours at room temperature (21°C to 25°C). • Reconstituted solutions with a preservative may be stored under refrigeration for up to 3 months, and up to 4 weeks at room temperature. • Intrathecal dilutions are stable at room temperature for 7 days, but it is generally recommended that they be used within 4-8 hours. • Reconstitution • Dilute powder with D5W or NS to a concentration ?25 mg/mL (20 mg and 50 mg vials) and 50 mg/mL (1 g vial). • Intrathecal solutions may be reconstituted to 2.5-5 mg/mL with NS, D5W, lactated Ringer's. Use preservative free preparations for intrathecal or high-dose administration. • Compatibility • Stable in D5NS, D5W, NS.
Methotrexate MOA • Methotrexate is an antineoplastic anti-metabolite. Anti-metabolites masquerade as purine or pyrimidine - which become the building blocks of DNA. • Methotrexate inhibits folic acid reductase which is responsible for the conversion of folic acid to tetrahydrofolic acid. • At two stages in the biosynthesis of purines and at one stage in the synthesis of pyrimidines, one-carbon transfer reactions occur which require specific coenzymes synthesized in the cell from tetrahydrofolic acid. Tetrahydrofolic acid itself is synthesized in the cell from folic acid with the help of an enzyme, folic acid reductase. • Methotrexate looks a lot like folic acid to the enzyme, so it binds to it quite strongly and inhibits the enzyme. Thus, DNA synthesis cannot proceed because the coenzymes needed for one-carbon transfer reactions are not produced from tetrahydrofolic acid because there is no tetrahydrofolic acid.
Calcium Leucoverin: • In the treatment of accidental overdosages of folic acid antagonists, LEUCOVORIN (calcium folinate) should be administered as promptly as possible. As the time interval between the administration of antifolate and LEUCOVORIN rescue increases, the effectiveness of LEUCOVORIN in counteracting toxicity decreases. Monitoring of the serum METHOTREXATE (MTX ) concentration is essential in determining the optimal dose and duration of therapy. Delayed MTX excretion may be caused by a third space fluid accumulation (i.e., ascites, pleural effusion), renal insufficiency, low pH of urine, or inadequate hydration. Under such circumstances, higher doses of LEUCOVORIN or prolonged administration may be indicated.
Mechanism Of Action: As leucovorin is a derivative of folic acid, it can be used to increase levels of folic acid under conditions favoring folic acid inhibition (following treatment of folic acid antagonists such as methotrexate). • A folic acid deficiency is produced during therapy with the folic acid antagonists, aminopterin and amethopterin (METHOTREXATE), used as antineoplastic agents and with the chemotherapeutic agent, pyrimethamine. • These agents competitively inhibit the conversion of folic acid to folinic acid. Their affinity for folate reductase is so much greater than that of folic acid that not even large doses of folic acid will correct the drug-induced deficiency. • In the event of a severe toxic reaction, the already reduced form, folinic acid, can be given, since it can be used directly to form new coenzyme.
In addition to calcium folinate administration, measures to ensure the prompt excretion of methotrexate are an integral part of the calcium folinate rescue treatment. These measures include: • a) Maintenance of urine output above 2,500 mL/24hr in adults by increased oral or intravenous fluids 12 hours before and for 36 hours after the end of methotrexate infusion. • b) Alkalinisation of urine so that the urinary pH is greater than 7.0 before methotrexate infusion. • c) Plasma methotrexate concentration and serum creatinine should be measured at least 24, 48, and 72 hours after the initiation of the methotrexate infusion. These measurements must be continued until the plasma methotrexate level is less than 10-7 molar (0.1μM). • Delayed methotrexate excretion may be seen in some patients. This may be caused by a third space accumulation (as seen in ascites or pleural effusion for example), renal insufficiency or inadequate hydration. See also section 6. Under such circumstances, higher doses of calcium folinate and/or prolonged administration may be indicated.
5)Cytarabin: • Storage • Powder for reconstitution: Store intact vials of powder at room temperature 15°C to 30°C (59°F to 86°F). • Reconstituted solutions are stable for up to 8 days at room temperature, although the manufacturer recommends use within 48 hours. • Solution: Prior to dilution, store at room temperature, 15°C to 30°C (59°F to 86°F); protect from light. • Do not refrigerate solution; precipitate may form. • Reconstitution • Reconstitute powder with bacteriostatic water for injection, bacteriostatic 0.9% NaCl. • For I.T. use: Reconstitute with preservative free diluent. • For I.V. infusion: Dilute in 250-1000 mL 0.9% NaCl or D5W. • Note: Solutions containing bacteriostatic agents should not be used for the preparation of either high doses or intrathecal doses of cytarabine; may be used for I.M., SubQ, and low-dose (100-200 mg/m2) I.V. solution. • Compatibility • Stable in D5LR, D51/4NS, D5NS, D10NS, D5W, LR, NS.