Download
1 / 38
550 likes | 1.5k Views
TETANUS. By Chandana Krishna 4 th term B.M.C. TETANUS. Tetanus is a medical condition characterised by prolonged contraction of skeletal muscle fibres. Introduction.

E N D
TETANUS By Chandana Krishna 4th term B.M.C
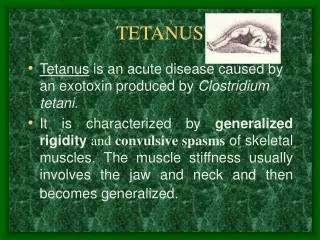
TETANUS • Tetanus is a medical condition characterised by prolonged contraction of skeletal muscle fibres.
Introduction • Primary symptoms by-tetanospasmin, a neurotoxin produced by the Gram-positive, obligate anaerobic bacterium Clostridium tetani. • Infection generally occurs through wound contamination, & often involves a cut or deep puncture wound.
Introduction • As the infection progresses, muscle spasms in the jaw develops, hence the common name, lockjaw. • This is followed by difficulty swallowing & general muscle stiffness & spasms in other parts of the body. • Infection can be prevented by proper immunisation & by post-exposure prophylaxis.
Clostridium tetani • Cl.tetani is widely distributed in soil & in intestine of human beings & animals. • They cause tetanus in both man & animal.
Morphology • Gram-positive, 4-8µm×0.5µm bacillus. • Has straight axis, parallel sides & rounded ends. • Occurs singly & occasionally in chains.
Morphology • It is capsulated & motile with peritrichate flagella (except typeVI Cl. tetani-nonflagellar strain). • Young cultures are strongly Gram positive but older cells show variable staining & may be even Gram negative.
Cultural characteristics • It is an obligatory anaerobe (grows only in absence of oxygen). • Optimum temparature-37°C & pH-7.4. • It grows on ordinary media.
Cultural characteristics • 1.Robertson’s cooked meat medium: turbidity & some gas formation. The meat is not digested but turns black on prolonged incubation. • 2.Blood agar: fine translucent film of growth.α hemolysis is produced, which later develops into β hemolysis, due to the production of hemolysin (tetanolysin)
Cultural characteristics • 3.Deep agar shake cultures: spherical fluffy balls, 1-3mm in diameter, made of filaments with radial arrangement. • 4.Gelatin stab culture: fir tree appearance with slow liquefaction.
Spore • The spores are spherical, terminal & bulging, giving the bacillus the characteristic ‘drumstick’ appearance. • Morphology depends on stage of development. • Young spore may be oval rather than spherical.
Biochemical reactions • Feeble proteolytic but no saccharolytic property. • Forms indole. • MR & VP negative. • H2S is not formed. • Nitrates are not reduced. • Gelatin liquefaction-slow. • Greenish fluorescence produced on media containing neutral red.
Resistance • Spore resistance to heat show strain variation. • Majority are killed by boiling for 15min. • Some withstand boiling for 3hr & dry heat at 160°C for 1hr. • Spores can survive in soil for years & are resistant to most antiseptics. • Not destroyed by 5% phenol or 0.1% HgCl2 solution in 2 weeks or more.
Susceptibility • Autoclaving at 121°C for 15min kills the spores readily. • Iodine(1% aqueous soon) and H2O2 (10 volume) kills spores within few hours.
Toxins • All types produce same toxins which are pharmacologically & antigenically identical. • Plasmid mediated. • 1.Tetanolysin • 2.Tetanospasmin
Tetanolysin • Heat & O2 labile hemolysin. • Cause red cell lysis. • Pathogenic role not clear. • May act as leucocidin.
Tetanospasmin • O2 stable & heat labile neurotoxin. • Good antigen & specifically neutralised by antitoxin. • Similar to botulinum toxin in str. • Gets toxoided spontaneously or in presence of formaldehyde.
Pathogenesis • Usual mode of infection-Penetrating injury. • Germination & toxin production occurs only in favorable condition-↓OR potential, devitalised tissues, foreign bodies, concurrent infection. • Resembles strychnine poisoning
Antigens • All strains share common somatic (O) antigen. • On basis of flagellar (H) antigen 10 types(Ι to X) are recognised by agglutination tests. • Type VI is non-flagellated strain.
1.Local tetanus • Persistent spasm of musculature at site of primary infection (injury site). • Contractions persist for weeks before subsiding. • Its generally milder, 1% cases are fatal but may precede the generalised tetanus.
2.Cephalic tetanus • Primary site of infection is head injury or otitis media. • Associated with disfunction of 1 or more cranial nerves, most commonly facial nerve. • Poor prognosis.
3.Generalised tetanus • Most common form(80% of cases). • Presents with a descending pattern. • 1st sign is trismus(lockjaw) -due to spasm of masseter muscles. • Followed by stiffness of the neck, difficulty in swallowing, rigidity of abdominal muscles.
Risus sardoricus • Characteristic sardonic smile in tetanus • Results from sustained contraction of facial muscles.
Opthisthotonus • Back spasm seen in tetanus
4.Tetanus neonatorum • It is the generalised tetanus that occurs in newborn infants. • Occurs in infants of non-immunised mothers.
Tetanus neonatorum • Occurs from infection of un-healed umbilical stump particularly when stump is cut with non-sterile instrument. • Very poor prognosis
Laboratory diagnosis • Diagnosis made based on clinical presentation. • Specimen: Wound swab, exudate or tissue from the wound. • 1.Direct smear & gram staining • 2.Culture • 3.Animal inoculation
Direct smear • Show Gram-positive bacilli with drum-stick appearance. • Morphologically indistinguishable from similar nonpathogenic bacilli.
Culture • Done in blood agar & aminoglycoside blood agar under anaerobic condition or in Robertson’s cooked meat medium. • Produces swarming growth after 1-2 days of incubation. • In contaminated specimen heat at 80°C for 10mins before culture to destroy non-sporing organisms.
Animal inoculation • To demonstrate toxigenicity. • Positive case : test animal develops stiffness & spasm of tail & inoculated hind limb within 12-24hrs which spreads to rest of the body. Death occurs in 1-2 days.
Prophylaxis • 1.Surgical attention • 2.Antibiotics • 3.Immunisation-passive,active or combined.
Surgical Prophylaxis • Aims at • removal of foreign bodies, necrotic tissue & blood clots, • To prevent an anaerobic envt favourable for the Clostridium tetanae
Antibiotic prophylaxis • Aims at destroying or inhibiting tetanus bacilli & pyogenic bacteria in wounds so that toxin production is prevented. • Long-acting Penicillin is the drug if choice. Erythromycin is an alternative. • Bacitracin or neomycin can be applied locally. • Has no action on toxin.
Immunisation • Combined immunisation: Tetanus immunoglobulin(TIG) & tetanus toxoid are given on different arms. • Provides both passive & long-lasting immunity.
Treatment • Isolate pt. from noise & light which may provoke convulsions. • Followed by supportive care. • TIG is infused. • Antibacterial therapy started.
Epidemiology • World wide distribution- higher in developing countries due to warm climate, unhygienic practices & poor medical services.
Prevention & control • By active immunisation with tetanus toxoid. 1.TT-2 doses for pregnant women, 2.DPT at 6, 10, 14 weeks after birth, 3.DPT booster at 18 months 4.DT at 5yrs. 5.TT boosters at 10 & 16 yrs.