Download
1 / 1
10 likes | 293 Views
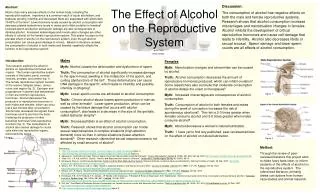
Screening of new admissions during period of study (N = 35). Screening of existing database (N = 49). Opioid only dependent participants (N = 51). Opioid and alcohol co-dependent participants (N = 33). Informed consent obtained. WPH Admission Assessment (Modified MAP)

E N D
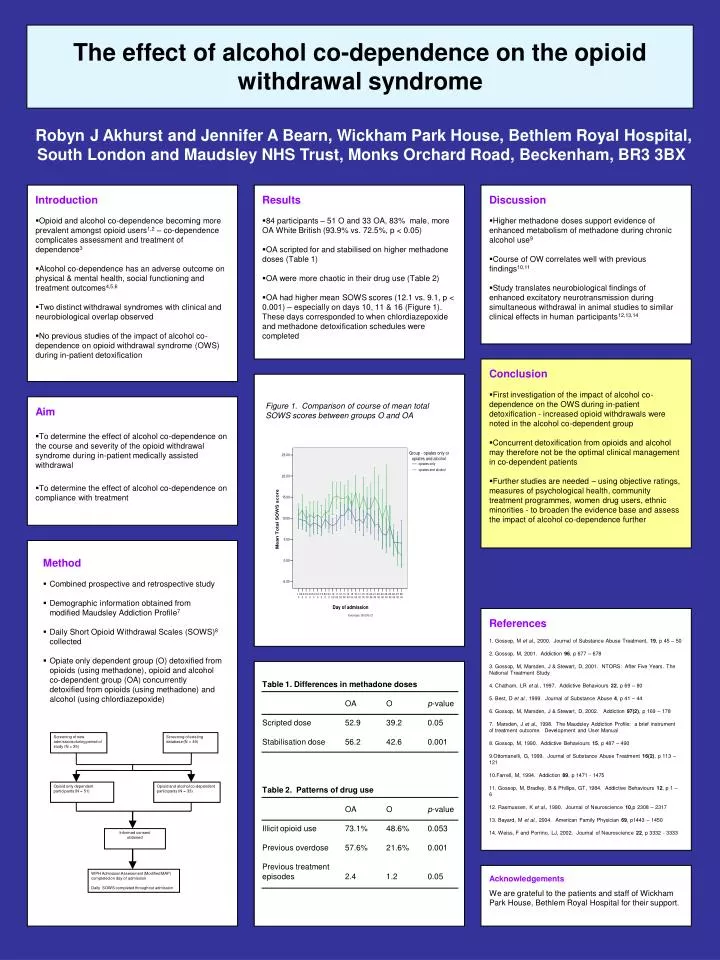
Screening of new admissions during period of study (N = 35) Screening of existing database (N = 49) Opioid only dependent participants (N = 51) Opioid and alcohol co-dependent participants (N = 33) Informed consent obtained WPH Admission Assessment (Modified MAP) completed on day of admission Daily SOWS completed throughout admission The effect of alcohol co-dependence on the opioid withdrawal syndrome Robyn J Akhurst and Jennifer A Bearn, Wickham Park House, Bethlem Royal Hospital, South London and Maudsley NHS Trust, Monks Orchard Road, Beckenham, BR3 3BX Introduction • Opioid and alcohol co-dependence becoming more prevalent amongst opioid users1,2 – co-dependence complicates assessment and treatment of dependence3 • Alcohol co-dependence has an adverse outcome on physical & mental health, social functioning and treatment outcomes4,5,6 • Two distinct withdrawal syndromes with clinical and neurobiological overlap observed • No previous studies of the impact of alcohol co-dependence on opioid withdrawal syndrome (OWS) during in-patient detoxification Results • 84 participants – 51 O and 33 OA, 83% male, more OA White British (93.9% vs. 72.5%, p < 0.05) • OA scripted for and stabilised on higher methadone doses (Table 1) • OA were more chaotic in their drug use (Table 2) • OA had higher mean SOWS scores (12.1 vs. 9.1, p < 0.001) – especially on days 10, 11 & 16 (Figure 1). These days corresponded to when chlordiazepoxide and methadone detoxification schedules were completed Discussion • Higher methadone doses support evidence of enhanced metabolism of methadone during chronic alcohol use9 • Course of OW correlates well with previous findings10,11 • Study translates neurobiological findings of enhanced excitatory neurotransmission during simultaneous withdrawal in animal studies to similar clinical effects in human participants12,13,14 Conclusion • First investigation of the impact of alcohol co-dependence on the OWS during in-patient detoxification - increased opioid withdrawals were noted in the alcohol co-dependent group • Concurrent detoxification from opioids and alcohol may therefore not be the optimal clinical management in co-dependent patients • Further studies are needed – using objective ratings, measures of psychological health, community treatment programmes, women drug users, ethnic minorities - to broaden the evidence base and assess the impact of alcohol co-dependence further Aim • To determine the effect of alcohol co-dependence on the course and severity of the opioid withdrawal syndrome during in-patient medically assisted withdrawal • To determine the effect of alcohol co-dependence on compliance with treatment Figure 1. Comparison of course of mean total SOWS scores between groups O and OA Method • Combined prospective and retrospective study • Demographic information obtained from modified Maudsley Addiction Profile7 • Daily Short Opioid Withdrawal Scales (SOWS)8 collected • Opiate only dependent group (O) detoxified from opioids (using methadone), opioid and alcohol co-dependent group (OA) concurrently detoxified from opioids (using methadone) and alcohol (using chlordiazepoxide) References 1. Gossop, M et al., 2000. Journal of Substance Abuse Treatment, 19, p 45 – 50 2. Gossop, M, 2001. Addiction 96, p 677 – 678 3. Gossop, M, Marsden, J & Stewart, D, 2001. NTORS: After Five Years. The National Treatment Study 4. Chatham, LR et al., 1997. Addictive Behaviours 22, p 69 – 80 5. Best, D et al., 1999. Journal of Substance Abuse 4, p 41 – 44 6. Gossop, M, Marsden, J & Stewart, D, 2002. Addiction 97(2), p 169 – 178 7. Marsden, J et al., 1998. The Maudsley Addiction Profile: a brief instrument of treatment outcome. Development and User Manual 8. Gossop, M, 1990. Addictive Behaviours 15, p 487 – 490 9.Ottomanelli, G, 1999. Journal of Substance Abuse Treatment 16(2), p 113 – 121 10.Farrell, M, 1994. Addiction 89, p 1471 - 1475 11. Gossop, M, Bradley, B & Phillips, GT, 1984. Addictive Behaviours 12, p 1 – 6 12. Rasmussen, K et al., 1990. Journal of Neuroscience 10,p 2308 – 2317 13. Bayard, M et al., 2004. American Family Physician69, p1443 – 1450 14. Weiss, F and Porrino, LJ, 2002. Journal of Neuroscience 22, p 3332 - 3333 Table 1. Differences in methadone doses OA O p-value Scripted dose 52.9 39.2 0.05 Stabilisation dose 56.2 42.6 0.001 Table 2. Patterns of drug use OA O p-value Illicit opioid use 73.1% 48.6% 0.053 Previous overdose 57.6% 21.6% 0.001 Previous treatment episodes 2.4 1.2 0.05 Acknowledgements We are grateful to the patients and staff of Wickham Park House, Bethlem Royal Hospital for theirsupport.