Download

1 / 32
350 likes | 534 Views
By: Rose Fontana BSN, RRNA and Courtney Henderson BSN, RRNA. The Effect of Intravenous Acetaminophen on Opioid Medication Requirements Following Cesarean Delivery. Acknowledgements. Webster University Committee Members: Michael Burns MS, CRNA Christopher Black MS, CRNA

E N D
By: Rose Fontana BSN, RRNA and Courtney Henderson BSN, RRNA The Effect of Intravenous Acetaminophen on Opioid Medication Requirements Following Cesarean Delivery
Acknowledgements • Webster University • Committee Members: • Michael Burns MS, CRNA • Christopher Black MS, CRNA • Jill Stulce PhD(c), CRNA • Phelps County Regional Medical Center
Cesarean Delivery (Martin et. al, 2013) • Most common surgical procedure performed in U.S. • 2012: 1,296,531 • Major abdominal surgery • High postoperative pain • Pain delays ambulation, mother-infant bonding, and decreases patient satisfaction
Postoperative Pain • Opioids: first line of treatment • Many adverse effects • Harmful to mom and possibly to baby • Delays bonding and ambulation • A multimodal analgesic regimen decreases the need for rescue opioids
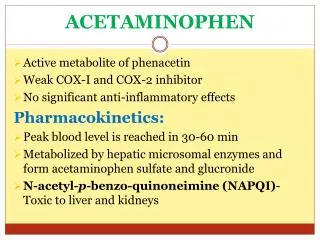
Acetaminophen (Mehta & Shah, 2010) • First synthesized in 1878 by Morse • First used in clinical practice in 1887 by Von Mering • N-acetyl-p-aminophenol • Non-salicylate antipyretic • Non-opioid analgesic
Acetaminophen(Mehta & Shah, 2010) • Mechanisms of Action- not fully understood • Inhibits prostaglandin synthesis • Serotonergic pathway activation • Cannabinoid receptor stimulation • N-methyl-D-aspartate receptor inhibition
Problem Statement • Even after spinal anesthesia and TAP blocks, patients continue to experience breakthrough pain in the early post cesarean delivery period. A multimodal analgesic regimen can decrease the amount of rescue opioid medications necessary for adequate pain control with less unwanted opioid side effects.
Purpose of the Study • The purpose of this study was to determine if the administration of intravenous acetaminophen following cesarean delivery leads to a decrease in postoperative opioid requirements
Hypotheses • Null Hypothesis: The use of intravenous acetaminophen in combination with a multimodal pain management regimen will not decrease postoperative opioid requirements after cesarean delivery • Alternative Hypothesis:The use of intravenous acetaminophen in combination with a multimodal pain management regimen will decrease postoperative opioid requirements after cesarean delivery
Phelps County Pain Management Protocol • Each cesarean delivery patient will receive: • Subarachnoid block with 0.75% bupivacaine in 8.25% dextrose • Intrathecal morphine 0.1mg • Intrathecal fentanyl 10-15 mcg • TAP block with 20-30 mL 0.5% ropivacaine • Ketorolac 30 mg every 6 hours for the first 24 hours postoperatively
Research Question Does intravenous acetaminophen decrease postoperative opioid requirements following cesarean delivery?
Research Design • Retrospective analysis of 329 patient charts • 145 cases during January 1, 2012-November 2012 • Control Group= No Acetaminophen • 182 cases during November 2012- December 31, 2013 • Experimental Group= 1 gram of IV Acetaminophen every six hours for 24 hours • The opioid medication consumption for each patient was totaled and converted to IV morphine equivalents using an opioid analgesic converter from GlobalRPH
Inclusion Criteria • Patients included in this study: • Females undergoing elective cesarean delivery • Each received entire pain management protocol: • Subarachnoid block with 0.75% bupivacaine in 8.25% dextrose • Intrathecal morphine 0.1mg • Intrathecal fentanyl 10-15 mcg • TAP block with 20-30 mL 0.5% ropivacaine • Ketorolac 30 mg every 6 hours for the first 24 hours postoperatively • Acetaminophen group also received 1 g of IV acetaminophen every 6 hours for the first 24 hours postoperatively
Exclusion Criteria • Exclusion criteria for this study included: • Failure to receive the entire pain management protocol • General anesthetic • ICU admission or another surgery within 24 hours • Contraindication to regional anesthesia • Additional gynecological surgeries • Emergency cesarean delivery
Non-Acetaminophen Group • 145 charts were reviewed • 40 charts were excluded due to an incomplete pain management protocol • 27 charts were excluded due to additional gynecological procedures • 13 charts were excluded due to conversion to general anesthesia, intensive care unit admission or additional surgery within 24 hours of cesarean delivery, or a multitude of factors • Total of 65 patients in the non-acetaminophen group
Acetaminophen Group • 184 charts were reviewed • 55 charts were excluded due to an incomplete pain management protocol • 26 charts were excluded due to additional gynecological procedures • 21 charts were excluded due to conversion to general anesthesia, intensive care unit admission or additional surgery within 24 hours of CD, or a multitude of factors • Total of 82 patients in the acetaminophen group
Statistical Analysis • Data was recorded in Microsoft Excel and converted for analysis using GraphPad Prism 5.0 • A significance level of p<0.05 was used in all analyses
Demographics • Age: No significant difference (p=0.2237) • BMI: No significant difference (p=0.8600) • Previous Cesarean Delivery: No significant difference (p=0.7319) • ASA I/II/III • Non-Acetaminophen Group- 2/60/3 • Acetaminophen Group- 4/74/4
Assumptions • Assumptions relative to this study include • All anesthetic procedures were performed and documented correctly • Opioid medications and intravenous acetaminophen were administered and documented accurately
Primary Findings: Mean Opioid Usage • Non-Acetaminophen: 3.33 mg of morphine • Acetaminophen: 3.07 mg of morphine
Results • Mean Morphine Consumption: • One-tailed t-test showed: • No significant decrease (p=0.3456)
Results • No statistically significant decrease in postoperative morphine consumption with the addition of IV acetaminophen to a multimodal pain management regimen following cesarean delivery • The results are not conclusive for a benefit of the addition of the IV acetaminophen • We accept the null hypothesis
Incidental Findings • Multimodal pain management protocol without acetaminophen • mean opioid consumption was 3.33mg • A study by Girgin, Gurbet, Turker, Aksu, and Gulhan • Intrathecal morphine 0.1-0.4mg + 0.5% bupivacaine • mean opioid consumption was 23.5mg • Supports use of this multimodal pain management protocol
Incidental Findings: • A total of 28 patients from both the non-acetaminophen and acetaminophen groups were excluded for no ketorolac administration • These patients’ morphine consumption was calculated and found to be greater than those that received the entire pain management protocol
Incidental Findings • n=147 all those included in the study • mean opioid consumption: 3.187 mg • n=28 no ketorolac • mean opioid consumption: 7.429 mg • A Welch’s correction was applied to a t-test to analyze significance • There was a significance found with p= 0.0043 • Although corrections were made for the variance in sample size, it makes the significance of the p value unreliable • cannot be considered dependable results • warrants further study
Incidental Findings • of the 28 that did not receive ketorolac • n=11 non-acetaminophen group • mean morphine consumption was: 6.955 mg • n=17 acetaminophen group • mean morphine consumption was: 7.735 mg • p=0.7814 • No significance that intravenous acetaminophen lowers postoperative opioid requirements in the absence of ketorolac
Future Recommendations • Perform a prospective randomized double-blind study evaluating the effect of ketorolac as part of a multimodal analgesic regimen post cesarean delivery • Incidental findings of this study suggest investigation of ketorolac efficacy would be advantageous
Limitations • Limitations for this study include • Only measured opioid consumption for 24 hours • Did not evaluate • pain scores • time to first ambulation • sedation scores • patient satisfaction • Retrospective: no influence on multimodal pain management regimen, already in place • dependent on staff to give appropriate postoperative doses • Intrathecal morphine shortage
Future Recommendations • Perform this study as a prospective randomized double-blind study with better controlled variables • Same surgeon and anesthesia provider placing the spinal and TAP block • The same postoperative opioid medications • Identical anesthetic and analgesic dosages
References • Martin, J., Hamilton, B., Ventura S., Osterman M., Curtin, S., & Mathews, T. J., (2013). Births: Final data for 2012. National Vital Statistics Reports; National Center for Health Statistics, 62(9), 1-87. • Mehta, V., & Shah, S. (2010). Paracetamol: the forgotten drug. British Journal Of Hospital Medicine (London, England: 2005), 71(11), 606-607. • Girgin, N., Gurbet, A., Turker, G., Aksu, H., & Gulhan, N. (2008). Intrathecal morphine in anesthesia for cesarean delivery: dose-response relationship for combinations of low-dose intrathecal morphine and spinal bupivacaine. Journal of Clinical Anesthesia, 20(3), 180-185.