Download
1 / 55
550 likes | 704 Views
Incontinence: A Crucial Conversation about the Skin on that Bottom Line. Laura Tidwell MSN 621 Alverno College April 2011. Navigation Tips. Move forward Move back Last slide Viewed Table of Contents “Compass” retrieved from Microsoft Windows 2007 Clipart

E N D
Incontinence: A Crucial Conversation about the Skin on that Bottom Line Laura Tidwell MSN 621 Alverno College April 2011
Navigation Tips Move forward Move back Last slide Viewed Table of Contents “Compass” retrieved from Microsoft Windows 2007 Clipart “Compass” retrieved from Microsoft Windows 2007 Clipart
Purpose Increase awareness of the pathophysiological factors that make Incontinence a concern for healthcare professionals, specifically nurses. “What we think determines what we see-even though it often seems the other way around” (Carlson, 2006, p. 13)
Objectives 1. Review skin Pathophysiology 2. Relate harmful effects of urine and feces due to incontinence. 3. Discuss Case Based patient Scenario, with multiple concerns, and how those concerns have implications for an incontinent patient. 4. Conceptualize inflammation processes and the risks as they relate to incontinence.
You are Here TABLE OF CONTENTS Case Study Diabetes at a Glance Common Disorders & Genetic Risk Epidermis & Dermis Neural Control of Incontinence Potential Complications Urine & Feces Risks for Incontinence Inflammation Stress Responses Case Study Outcome Moisture Lesions Elderly patients at Risk Click Topic to Learn More
Case Study One of your 4 patients is an 82year old woman, admitted with increased confusion and failure to thrive. She is a Type 2 Diabetic with a Stage 1 ulcer on her R buttock and a Stage 2 ulcer on her L buttock. She has Ensure ordered 3 X Daily with meals to help supplement her nutritional needs. Her activity level is up to chair 3 X Daily with meals. She transfers with assist of 2. The totalrecorded intake in the last 24 hours is: 50cc between 0000-0759, Zero between 0800-1559, 100cc between 1600-2359 which adds up to 150cc. When you enter the room at 3 pm she is sleeping in her chair, she has been up since lunch at 1200and has not been toileted since 1130 am, she wears a depends. There has been zero recorded outputin 24 hours. • “Nurse” retrieved from Microsoft Windows 2007 Clipart
Focus on Our Patient “Normal” Urinary output = 30-60cc per hour. Zero Output Recorded past 24 Hours If the patient is Incontinent does that mean we don’t track her output? . Cc=ml 1 Ensure = 355cc 150cc=less than 1/2 can Ensure 3 X daily orders 150cc Input Recorded Past 24 Hours Stage 1 & Stage 2 pressure ulcers Patient is Diabetic Is Incontinence Normal? Urinary Incontinence is widely accepted as “normal”, it can often be cured and it can always be relieved by good management “Confusion” retrieved from Microsoft Windows 2007 Clipart
MoistureWhat is a Depends Purpose in life? Hold Moisture in, Right? Excessive and continuous skin moisture can pose a risk to compromise the integrity of the skin by causing the skin tissue to become macerated and therefore be at risk for epidermal erosion. superficial, partial skin loss and shiny wet skin caused by by incontinence McDonagh, D. (2008). Moisture lesion or pressure ulcer? A review of the literature. Journal of Wound Care, 17(11), 461. Retrieved from EBSCOhost, February 28, 2011. Permission granted.
The motor component of the neural reflex that causes bladder emptying is controlled by the Parasympathetic Nervous System. Stimulation of Parasympathetic neurons (the bladder fills) = Contraction of detrusor muscle = urination (Misconception Junction, 2010) Permission granted under Wikimedia Commons (Porth, 2009)
Parasympathetic Control /Incontinence This is mediated by acetylcholine. Receptors that respond to acetylcholine are called Cholinergic Receptors There are receptors found in the parasympathetic endings of the detrusor muscle. The detrusor muscle is the 2nd layer in the lining of the bladder, made up of smooth muscle fibers. “Muscle Fiber” retrieved from Microsoft Windows 2007 Clipart (Porth, 2009)
Sympathetic promotes bladder filling FDOH, 2010. Permission Granted
Sympathetic Control/Incontinence The relaxation and storage function of the bladder is controlled by the Sympathetic Nervous System. Stimulation of sympathetic neurons = Relaxation of detrusor muscle The bladder is supplied with a1and B2 adrenergic receptors. The B2 receptors are in the detrusor muscle and they relax it, until the volume when the micturition (passage of urine) reflex is triggered by the increasing bladder volume. The activation of a1 receptors produces the contraction of the internal sphincter. (Porth, 2009)
Sympathetic or Parasympathetic? Receptors found in Detrusor Muscle are responsible for Urination Parasympathetic Were you right? Receptors are responsible for Relaxation (filling) of bladder Sympathetic Click in Above Boxes (Author, N., 2011) Permission granted under Wikimedia Commons
Common Disorders Stroke &Advanced Age Loss of ability to perceive bladder filling Parkinson disease (Commonly Genetic) Detrusor contractions are elicited suddenly Spinal cord Injury Storage reflexes are provoked during filling Click in boxes to learn more (Porth, 2009)
Common Disorders Injury to sacral cord or spinal roots Bladder fills but does not contract Pelvic Surgery Increased filling and impaired sphincter control Diabetic neuropathies & Multiple Sclerosis Bladder overfilling occurs due to a loss of ability to perceivebladder filling Click ON Frame to learn more (Porth, 2009)
Risks for Incontinence: Studies have suggested a genetic component of Stress Urinary Incontinence and Pelvic Organ Prolapse(Allen, 2010). Possible link to genetics predisposing patients to recurrent UTIs which can be a contributing factor (especially in elderly) to urinary incontinence (Zaffanello, et al., 2010). Endocrine Bladder stasis and infection are long term complications of Diabetes Mellitus (Which our patient has) Atropic Vaginitis An inflammation of the vagina (and the outer urinary tract) due to the thinning and shrinking of the tissues. This is all due to a lack of the reproductive hormone estrogen, which happens naturallyduring peri-menopause, and increasingly so in post-menopause. (Author, N. 2010) (Porth, 2009)
Muscle control: Role in Incontinence FDOH, 2010. Permission Granted
Back to Skin About the barrier it forms Intact skin forms a physical barrier with its closely packed cells, multiple layering, continuous shedding of cells and presence of protective keratin (Porth, 2009) About bacteria on the skin The skin has simple chemicals that create a salty, acidic environment and antibacterial proteins, such as enzymes that inhibit the colonization of microorganisms and aid in their destruction (Porth, 2009) Can this barrier be broken? Some pathogens can penetrate the anatomic layers and cause physiologic changes that result in infectious disease (Porth, 2009) Click boxes to learn more
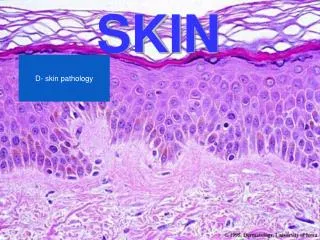
Stained slide at 10x of normal Epidermis and Dermis Epidermis (Physical Barrier) Closely packed cells, multiple layering (Kilbad, 2008) Permission granted under Wikimedia Commons
Focus on the Dermis Vasculature (US-Gov.2005-2009). Permission granted under Wikimedia Commons. .
Epidermis & Dermis Epidermis Body’s 1st line of defense Prevention of: pathogenic organisms, excessive water loss Dermis Connective tissue layer that separates the Epidermis from the Subcutaneous fat layer. Supports the Epidermis and is the Primary source of nutrition. Blood Vessels are within this layer. (Vasculature) within this layer The arterial vessels nourish the skin. The Dermis is well supplied with Sensory Neurons The skin is the largest organ of the body, it is about 2 mm thick and weighs approximately six pounds.
The Dermis Layer of Skin…….Do you know? Click boxes to test your knowledge! The Blood Vessels are within this Layer Yes! The Blood Vessels are within this Layer! Is Well Supplied with Sensory Neurons Yes! Sensory Impairment happens at this level! Is the body’s 1st line of defense No….that is the Epidermis (Kilbad, 2008) Permission granted under Wikimedia Commons
Basics of Skin Assessment Sensory Perception Measures a patients' ability to detect and respond to discomfort or pain, their ability to cognitively react to pressure-related discomfort. Do you remember what our patient was admitted with? Click to check your answer Increased confusion & Failure to Thrive How long has she been up to the chair? 3 hours And…..she has an existing Stage 1 to her R buttock, Stage 2 to her L buttock (Click box)
Lets talk……Urine & Feces Urine is slightly acidic, it contains urea, sodium chloride, and organic salts, all of which can irritate the skin. Feces is waste from the Digestive Tract. It consists of foodresidueand bacteria. Imagine that on your skin! Fecal Incontinence is associated with an increased risk of skin damage. The alkali (increased pH), bacterial and enzymatic content of fecal material may irritateand damage the skin (Hurnauth, 2011) . Fecal incontinence left untreated can lead to excoriation and breakdown which may become infected. (Author, N. 2008).
We mentioned Enzymes, pH &Bacteriain Feces Enzymes are proteins that are made from amino acids, and they work to facilitate chemical reactions. The elevated pH of stool increases the activity of proteases and lipases (both are enzymes) found in stool, which causes increased permeabilityof the skin, which makes it more susceptible to other agents such as bile salts (found in urine). That’s IF our patient was Incontinent of Feces….. As for Bacteria, remember this? Some pathogens can penetrate the anatomic layers and cause physiologic changes that result in infectious disease
Urinary & Fecal Moisture Moisture lesion: superficial, partial skin loss, multiple irregular shaped spots and shiny wet skin caused by urinary incontinence Combined lesion: irregular wound shape, grade III pressure ulcer and moisture lesion Grade IV pressure ulcer and moisture lesion caused by unrelieved pressure and fecal incontinence McDonagh, D. (2008). Moisture lesion or pressure ulcer? A review of the literature. Journal of Wound Care, 17(11), 461. Retrieved from EBSCOhost, February 28, 2011. Permission granted.
Compounding the Risks of Incontinence Activity Level of physical activity, very little or no activity can encourage breakdown of tissue. Mobility Capability to adjust body position independently. Friction and Shear The amount of assistance needed to move, the sliding motion can cause shear which means the skin and bone are moving in opposite directions . Click box Restricted Mobility She requires assist of 2 to get up, this restricts her ability to toilet herself
Which area of Skin Breakdownis likely to be related to Incontinence? Absolutely! How did you know? This is a Pressure Ulcer, though it will be complicated by Incontinence it is caused by pressure Click on area of breakdown in picture, likely due to Incontinence (Author, N., 2011) Permission granted under Wikimedia Commons
If our patient was incontinent, then is she at risk for Inflammation? Inflammation is the body’s response to immune reactions, injury, or ischemic damage. Microbes Epithelial Barriers The classic response to inflammation includes redness, swelling, heat, pain or discomfort, and loss of function (Porth, 2009)
1st -The Vascular Stage of Inflammation Involves (Opening of capillary beds) which results in: • Arterioles Vasodilation Redness & Warmth • The area becoming congested • (Edema) (Porth, 2009)
Summary of Vascular Stage • Protein rich fluid (exudate) into extravascular spaces • Increased concentration of blood constituents (red cells, leukocytes, platelets, and clotting factors) • Stagnation of flow • Clotting of blood at the site of injury aids in the spread of infection • The osmotic pressure causes fluid to move into tissues producing: Increased permeability of microvasculature That leads to: Pain Impaired Function Swelling (edema) (Porth, 2009)
Next Stage: Cellular Inflammation Because they received the message from the chemical mediators that were released Chemical Mediators released from tissue cells Neutrophils migrate from blood vessels to the inflamed tissue (Histamine) from Basophils Macrophages Phagocytic leukocytes (WBCs that kill the bacteria or eat it) move into the area of injury or infection Neutrophils Become Macrophages once they move from the blood into the tissue Macrophages now present the antigen to other cells in hopes of finding a cell that will recognize the antigen Monocytes All photos: (Author, N., 2011) Permission granted under Wikimedia Commons (Porth, 2009)
Vascular or Cellular Stage? Exudate is produced in the _______ Stage of Inflammation: Cellular Try again, WBCs move into the area during this stage Vascular Great Job! ? Painis typically experienced during the _________ Stage of Inflammation: Cellular Try Again Vascular Nice Job! Fluid moves into tissues causing Pain ?
Stress Responses are the body's way of fixinga problem such as this one: Tissue Damage Release of Prostaglandins & Leukotrines Mast cells release Histamine & Acetylcholine (inflammatory mediators) Leads to: And Which causes Increased venule permeability Capillary endothelium adhesive proteins Vasodilation > WBCs and and and Then: Exudate leaks out of venules into tissues Then Release cytokines to attract more WBCs & promote healing WBCs adhere to capillary lining And Results: Decreased blood volume Tissues Swell: edema So they can: Phagocytize invading organisms + injured cells Causing: Pressure on nerves causes pain
Multiple Ways Body Responds to Stressors A decrease in the blood flow to kidneys (decreased volume due to poor PO intake) Stress Response Causes Kidneys to release Renin Confines blood flow to inner core of body and Subcutaneous tissue Vasoconstriction to Skin Stimulates Angiotensin 1 production Increase in Blood volume Vasoconstriction to kidneys Angiotensin 1 Converting Enzyme (ACE) converts it to Angiotensin 11 Na/K+ ATPase in distal tubule activated Adrenal Cortex releases Aldosterone
That's not all….. The Sympathetic Nervous System is turned on: Adrenal medulla Releases Epinephrine Hypothalamus releases Cortico-Releasing Hormone (CRH) Inflammation and immune responses are suppressed Maintaining Blood Glucose is the Body’s goal Cortisol (promotes glucose production by liver) Adrenal Cortex releases Cortisol Which blocks prostaglandin production, injured tissue can’t call WBCs
Glucose at a glance Glucocorticoids are produced in response to stress and are necessary for survival. They suppress the inflammatory response. Remember, maintaining the blood glucose is the body’s goal. Cortisol is a glucocorticoid, it stimulates glucose production by the liver, promotes protein breakdown and causes mobilization of fatty acids. As body proteins are broken down, amino acids are mobilized and transported to the liver, where they are used in the production of glucose (glucogenesis), this is the body’s way of producing energy. . “Magnifying Glass” retrieved from Microsoft Windows 2007 Clipart
Intake & Diabetes In a person with diabetes, the body raises the blood glucose but they are unable to utilize that energy depending on the type/severity of their disease,due to the body’s specific problem with making or utilizing insulin. Insulin is the only hormone known to have a direct effect on lowering Blood Glucose levels. It promotes glucose uptake by cells (for energy). Lets summarize: So the body can produce glucose for energy, even if her POintake is inadequate in response to stress. But………. in a Diabetic, the Glucose that was produced for energy cannot be utilized properly, in addition to the Immune Response being suppressed by the Cortisol production? (Porth, 2009) “Injection” retrieved from Microsoft Windows 2007 Clipart
Our Patient is a Type 2 Diabetic with a Stage 1ulcer on her R buttock and a Stage 2 ulcer on her L buttock What happens to our patient when the sympathetic nervous system is turned on? Remember the SNS turns on when chemical mediators are released from the cells (cellular stage of inflammation). Impaired healing Yes!!! That is NOT what we want for our patient! She will heal faster No, energy is taken away from inflammation and immune responses when the SNS is activated Increased BLOOD Glucose Great! Inflammation and immune responses are suppressed Impressive!!!
What is…Systemic Inflammatory Response (Sirs) SIRS is a serious condition related to systemic inflammation. There is an abnormal regulation of various cytokines Cytokines stimulate the migration and activation of the immune and inflammatory cells They are produced by those Macrophages we talked about, they recruit and direct migration of immune and inflammatory cells. They also affect the thermoregulatory center in the hypothalamus to produce fever, the most obvious sign of an acute phase response They are used extensively in intercellular communication. In addition, cytokines activate those cells, stimulating them to produce more cytokines Click boxes to learn about Sirs (Porth, 2009)
Sirs & our patient When there is a “Cytokine Storm” what do you think is happening? Does this seem a potential complication for a patient with Incontinence? There’s an abnormally high amount of cytokines being produced which could indicate SIRS RIGHT! There may be a rise in patient’s Temperature RIGHT AGAIN! Yes Absolutely! She has a portal of entry for invading organisms with skin breakdown No Try Again, does this patient have a breakdown in her Skin Barrier?
Fever In the ElderlyDoes this relate? Latesign of infection Slight elevations may indicate serious infection or disease They often have a lower baseline temperature They often increase their temperature during an infection but it may fail to reach a level that is equated with significant fever It has been suggested that 20%-30% of elders with Serious Infection present with an absent or blunted febrile response (Porth, 2009) “Elderly” retrieved from Microsoft Windows 2007 Clipart
Speaking of Elderly Slower reepithelialization of open wounds More Vulnerable to: • Chronic Wounds • Diabetic Wounds • Ischemic Ulcers Due To: • Immobility • Diabetes Mellitus • Vascular Disease“Elderly” retrieved from Microsoft Windows 2007 Clipart • Slower Healing Processes Was our Patient Elderly? Changes in the Micturition cycle that accompany the aging process makes the Elderly population more prone to Incontinence.
As if all that weren’t enough to think about…. Diuretics: Increased excretion of Sodium & Chloride in Urine = Higher Acidity Tranquilizers, Hypnotics: Side effects include: Increased Urinary Retention, Incontinence Antidepressants: Side effects include Nocturia, Frequency of Urination Anticholinergic: Prevent acetylcholine from combining with parasympathetic receptors Click in boxes to learn more about medication effects (Spratto & Woods, 2003, pp. 19-161)
Good News! Medications usually cause Transient Urinary Incontinence-Temporary It is believed that approximately 30% of all cases of urinaryincontinencein older people are transient. “Urinary Incontinence is widely accepted as “normal” in old age, although its consequences are devastating; it can often be curedand it can always be relieved by good management” (Ham & Sloane, 1997, p. 323)
How is our Patient doing? One of your 4 patients is an 82 year old woman admitted with increased confusion and failure to thrive. She is a Type 2 Diabetic with a Stage 1 ulcer on her R buttock and a Stage 2 ulcer on her L buttock. She has ensure ordered 3 X Daily with meals that she doesn’t like. Her activity level is up to chair 3 X Daily with meals. She transfers with assist of 2. The total recorded intake in the last 24 hours is: 50cc between 0000-0759, Zero between 0800-1559, 100cc between 1600-2359. When you enter the room at 3 pm she is sleeping in her chair, she has been up since lunch at 1200 and has not been toileted since 1130 am, she wears a depends. There has been Zero recorded output in 24 hours. Now she has a Temperature of 99.9 when her vitals are taken. She denies pain in the area of her pressure ulcers. She is assisted back to bed and the dressing to the L buttock which is saturated, is removed. The wound is cleaned and the bandage replaced.
On the way home from work…… The Nurse remembers that heat is a sign of inflammation, the patient’s temperature is rising which could indicate: Systemic Inflammation She thinks about the possibility that the patient cannot relate any sensation of pain in the areas of skin breakdown, due to: Sensory Impairment And begins to wonder if the next nurse will notify the physician of the discharge during her dressing change because this could indicate: Infection Click links to Learn More
Putting it all together Did the patients’ diet have significant implications in maintaining her health status? If our patient was incontinent, was it important for us to know that? Are Elderly patient’s at higher risk for complications from Incontinence? Risk factors for a Systemic Inflammatory Response? Yes to all (Click) Congratulations! Your patient is in educated hands! “Driving” retrieved from Microsoft Windows 2007 Clipart
The Next Day For the Nurse caring for this patient, it is Friday. For the patient that suffered a systemic inflammatory response, a poor outcome could have been prevented. How can we manage all those factors? ASSESSpatient’s Skin on Admission ,Q Shift & PRN Accurate Documentation of I & O Toilet patient regularly, in an effort to: Prevent Incontinence Recognize signs/symptoms of inflammation Report changes in discharge/drainage to physician Maintain or increase Nutritional status Click boxes to learn More
Was our Patient Incontinent? An estimated 15-30% of community-dwelling elders and 50% of institutionalized elders have severe urinary incontinence (Porth, 2009). 30% of this group also experience fecal incontinence (Ham & Sloane, 1997) The economic and social costs, annually, more than $3 billion is spent managing incontinence in nursing homes alone (Porth, 2009, p. 889) Incontinence increases social isolation, frequently leads to institutionalization of elderly persons, and predisposes to infections and skin breakdown (Porth, 2009, p. 889) Thank you for watching, I hope that you’ll consider the Potential Complications, involved in Incontinence and the Bottom Line for your patient.






![Designing the Conversation [SmashingConf 2016]](https://cdn4.slideserve.com/7568510/designing-the-conversation-dt.jpg)