Download
1 / 113
1.16k likes | 1.5k Views
SKIN AND MELANOMA. Radiation Therapy 4412 Radiation Oncology II. Overall Perspective. The skin is continually subjected to many external influences, making it susceptible to trauma, infection and disease. I. EPIDEMIOLOGY. Skin cancer is the most common type of human malignancy.

E N D
SKIN AND MELANOMA Radiation Therapy 4412 Radiation Oncology II
Overall Perspective • The skin is continually subjected to many external influences, making it susceptible to trauma, infection and disease.
I. EPIDEMIOLOGY • Skin cancer is the most common type of human malignancy. • Almost 1 million cases of skin cancer occur in the United States each year.
THREE MAJOR TYPES OF SKIN CANCER • 1. BASAL CELL • 2. SQUAMOUS CELL • 3. MALIGNANT MELANOMA
Most skin cancers will be either basal or squamous cell. • Also known as non-melanomas • They grow slowly • Spread little • Nearly 95% can be cured
BASAL CELL CARCINOMA • Makes up approx. 75% of all skin cancers • Commonly found on face and ears • Is seen on young and older persons • Slow growing, usually does not spread or invade • Yearly follow-ups • Develop a new tumor 3-5 years.
SQUAMOUS CELL • 20% of all skin cancers • Sun exposed areas of the body • Can develop within scars and ulcers • More aggressive than basal cell • Can spread to distant parts of body • Patient needs to be checked yearly • Can develop tumor in 3-5 years
MELANOMA • Less common than basal or squamous • Dangerous, can be life-threatening • Found in cells that produce melanin • White men- trunk of body • White women- lower leg • African-Americans- hands, skin under soles of feet (although rare)
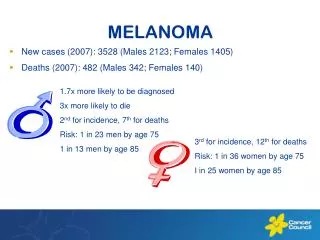
MALIGNANT MELANOMA • Is on the rise in the United States • 68,130 new cases (2010) • Incidence has been dropping since 1990’s for those younger than 50 • Increasing for those older than 50 • Due to: “healthy tans” skimpy clothing trends depletion of the ozone layer
Death rates have increased over the past 40 years. • 8,700 deaths (2010) • Overall 5 year survival rate for localized disease is 96% • About 82% of melanomas are diagnosed in a local stage.
100% curable if diagnosed early • Can spread to distant parts of the body • Makes up 5% of skin cancers • 75% of skin cancer deaths
Four Classifications of Malignant Melanoma • Superficial Spreading Melanomas (SSMs) • Nodular Melanomas (NMs) • Lentigo Malinga Melanomas (LMMs) • Acral Lentiginous Melanomas (ALMs)
Superficial Spreading Melanomas • “Radical Spreading Melanomas” • Most common subtype • Arise on anatomical site • Horizontal growth patterns • With time will grow vertically
Nodular Melanomas • Lump that grows quickly 6-18 months • Extends vertically into the skin • Occur at any site on the body • 2x more common in men than women • Ulcerate
Raised lesions • Vary in color • Very lethal-lack a radial growth phase • Invade early and frequently
Lentigo Maligna Melanomas • “Hutchinson’s freckles” • Chronic sun exposed areas • Older white females • Benign radical growth phase may last for decades • Might enter into vertical growth phase
Acral Lentiginous Melanomas • Found on palms, soles, nail beds, mucous membranes • Most common in black and oriental populations • Tan or brown or brown flat stain on palms or soles • Brown to black discoloration under nails • Often mistaken for a fungal infection
Prognostic Factors for Malignant Melanoma • Tumor thickness-thicker-poorer prognosis • Dept of invasion-deeper-poorer prognosis • Ulceration-worse prognosis • Lymph node status-positive lymph nodes • Metastatic status-poor prognosis
Gender- women do better than men before mets • Location of primary tumor • extremities including feet best prognosis • head and neck- some what worse • trunk- worse
Tendencies for people to develop skin cancers and melanomas can be grouped into the following categories:
GEOGRAPHICAL LOCATION • Higher chance of skin cancer nearer the equator • Sun’s rays are intense and direct • High altitudes- less atmosphere to filter sun’s rays.
SKIN TYPE • Fair complexion • less melanin • freckles • light colored eyes • red or blonde hair • Celtic background, Irish and Scottish • Nonmelanoma UV related is rare in African American
MULTIPLICITY(prior skin cancer occurrence) • Same carcinogen exposure as previous skin cancer • Weakness in immune system • Previous melanoma increases risk 5-9%
GENDER • Men have a higher skin cancer rate than women • Men work outside more often than women • Men are not as concerned about their skin as women
Farmers, construction workers, boaters, golfers, sunbathers and other outdoor sports and work are at the highest risk of developing skin cancer.
AGE • Average age for melanoma is 50 • Rarely occurs in childhood • Becoming more common among young people • Children or teens who have had severe, blistering sunburns • Develop from mid-teens and up
1. OVEREXPOSURE TO SUNLIGHT • Main cause of skin cancer • 90% of all skin cancers are caused by ultravioloet light • Sun’s rays are strongest between 10 am and 4 pm • Effects of sun exposure are accumulated over a lifetime
THREE TYPES OF UV RADIATION: • UVA • UVB • UVC
UVA (ultraviolet alpha rays) • remain relatively constant strength throughout the year • UVA rays penetrate the skin at deeper levels • Are less noticeably absorbed
UVA AND TANNING • UVA will cause some tanning • Will contribute to premature aging and wrinkling • Adverse skin reactions (photosensitive drugs) • Certain types of skin cancer
TANNING CONT’D • Tanning booths advertise UVA as safe • Doesn’t cause burning or reddening • Does penetrate • Just as dangerous as other UV’s
UVB- ULTRAVIOLET BETA • Called the “burning” ray • Quickly causes erythemia • More intense during summer months • At high altitudes • Close to the equator
UVB CONT’D • Most commonly associated with sunburns • and skin cancer • Also promotes premature aging and wrinkling
The short term results of unprotected exposure to UV rays are tanning and sunburn. • A sunburn causes: • skin redness • tenderness • pain • swelling • blistering
Symptoms of more serious sunburn include • fever • chills • upset stomach • confusion
The damage of UV radiation can include: • early wrinkling of the skin • skin cancer • melanoma • cataracts • loss of night vision • increased sensitivity of the skin
2. OCCUPATIONAL EXPOSURE • Coal tar • arsenic • pitch • creosote • radium
3. THERAPEUTIC OR OCCUPATIONAL EXPOSURE • After exposure to radiation- risk is up 20% • Latent period after initial exposure can be up to 50 years
BASAL CELL • Exposure to arsenic (used in medicines and poisons) • Therapeutic or occupational exposure to radiation • Xeroderma pigmentosum- genetic • Basal cell nevus syndrome-genetic • Multiple basal cell carcinomas of the skin, cysts of the jaw bones, pitting of the palms and soles and skeletal anomalies.
SQUAMOUS CELL • Human papilloma virus • Immunosuppression] • Thermal or electrical burns (chronic heat exposure) • Scars or inflammatory conditions
Etiology cont’d • Hydrocarbons from coal and petroleum • Areas of chronic drainage • Smoking, squamous cell carcinoma of the lip. • Has been linked to development of squamous cell in other anatomical areas.
MALIGNANT MELANOMA • Change in moles (nevus, nevi) • Congenital melanocytic nevi, present at birth • Common acquired nevi • Number of moles • Family history