Download
1 / 19
200 likes | 514 Views
Heparin in CRRT. Benan Bayrakci , 2014. McLean. Inactive Thrombin ( IIa ). Antitrombin 3. V, VIII, XIII, Fibrinogen. Heparin Binds to Antithrombin III and Speeds up its action by a 1000-fold. Inactive Factor Xa. Antitrombin 3. Common Pathway. Inactive Factor IXa , XIIa.

E N D
Heparin in CRRT Benan Bayrakci, 2014
Inactive Thrombin (IIa) Antitrombin 3 V, VIII, XIII, Fibrinogen Heparin Binds to Antithrombin III and Speeds up its action by a 1000-fold Inactive Factor Xa Antitrombin 3 Common Pathway Inactive Factor IXa, XIIa Antitrombin 3 Contact activation Pathway Also • Releases Tissue factor pathway inhibitor form endothelium • Binds to platelets and inhibits platelet aggregation
UFH is made up of heparin moleculesof varied sizes (5–30 kDa). Larger fragments:Anti-IIaactivity and are clearedrapidly (measuredbyAPTT) Smaller fragments: InhibitXa(normal APTT because of its delayed clearance)
Protocols • Heparin infusion prior to filter • Bolus with 10-30 units/kg • Infuse heparin at 5-20 units/kg/hr • Postfilter ACT measurement • Adjust post filter ACT 180-200 secs • Interval of checking is local standard and varies from 1-4 hrincrements
Monitoring • Anticoagulanteffect • Filter efficacy • Circuit life • Complications • Efficacy of UFH for prolonging filter life is proportional to the APTT and not to the heparin dose • APTT is maintained between 34–45 seconds, or anAPTT of 1.5–2.0 times normal
Advantages • Most commonly usedanticoagulant worldwidefor CRRT • Widely available • Simpleto monitor • Inexpensive • Familiarto physicians • Easytoadminister • Reversible with protamine
Disadvantages • Unpredictable andcomplex pharmacokinetics resulting in dosingvariability • Heparin-inducedthrombocytopenia • Heparin resistance because of lowpatient antithrombin levels • Risks ofhemorrhage (bleeding episodes: 10–50%, mortality 15%)
RegionalUnfractionatedHeparin–Protamine • Anticoagulant effects are restricted tothe circuit, lower risk ofbleeding • Difficulty in estimating theamount of protamine required • Initialratio of 100 between prefilterheparin (in units) and postfilter protamine (in mg) • Subsequent adjustmentaccording to APTT • Requiresmeasurement of both circuitand patient APTT • The heparin–protamine complex is taken upby the reticuloendothelial system and broken down, then heparin and protamine are released back into thecirculation • Protocols are cumbersome and difficultto standardize • Protamine infusionis associated with hypotension, anaphylaxis,cardiac depression, leukopenia, and thrombocytopenia
LowMolecularWeightHeparins • Havehigher anti-Xa • Pharmacokinetics is more predictable becauseof less plasma protein binding • More reliable anticoagulant response • Lowerincidence of HIT • Reversalwith protamine is less effective • Dalteparin, enoxaprin, and nadroparin have been studiedin CRRT • Excretedrenally, theireffects are prolonged in renal failure • Special coagulationassays are required to monitor anti-Xaactivity
Longerfilter survival times, andlower cost, bleedingcomplications not increasedDetermination of anti-Xa levels aimingat 0.25–0.35 IU/ml is recommended
174 patients No significant difference in survival up to day 30Thereweremoremetabolicdisturbances withcitrateanticoagulation
Regional anticoagulation with citrate does not eliminateany need for heparin since, manyother indications for systemic anticoagulation may emergeduringtherapy Citrateanticoagulation has distinct advantages withregard to haemofilter patency and the risk of HIT andbleeding
Neithercitratenorheparin anticoagulation should be regarded as a therapeuticstandard, since there is no advantage of one of these substanceswith regard to patient mortality. Forpatientswhoare at low risk of bleedingand do not haveothercontraindicationstoheparinsuchas HIT, considerusing UFH Forpatientswhoare at high risk forbleedingandwho do not haveliverfailure, considerusingregionalcitrateanticoagulation
The ideal anticoagulantshouldprovide • Optimal anti-thromboticactivity • Minimal bleedingcomplications • Negligiblesystemiceffects • Inexpensive • Havea shorthalf-life • Can be easilyreversed • Monitoringmethodsshouldbe simpleandavailable
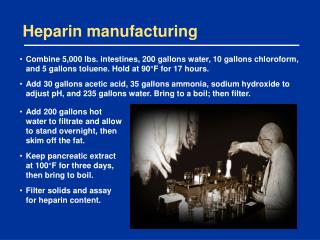
Heparinwasusedto be manufactured in factoriesfromporcineintestine or bovine lung