Download
1 / 52
520 likes | 526 Views
Learn about the functions of the urinary system, including removing nitrogenous wastes, maintaining electrolyte balance, and regulating fluid levels in the blood. Explore the anatomy of the kidney and the process of urine formation. Understand the role of hormones in kidney function. Discover how the urinary system helps maintain chemical homeostasis in the body.

E N D
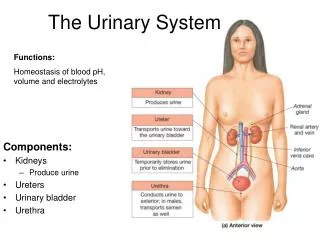
Functions • Remove nitrogenous wastes • Maintain electrolyte, acid-base, and fluid balance of blood • Homeostatic organ system • Acts as blood filter • Release hormones: calcitriol & erythropoietin
Nitrogenous Wastes urea uric acid ammonia
The Urinary System Maintaining Chemical Homeostasis
blood filtration tubular reabsorption and secretion General Functioning of the Kidney “refreshed” blood urine
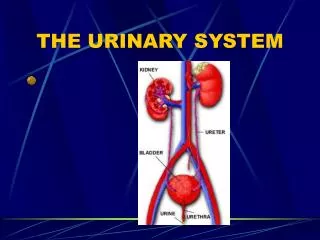
kidneys ureters urinary bladder urethra Organs of the Urinary System
renal pyramids renal pelvis renal cortex renal capsule ureter renal medulla Kidney Anatomy
nephron renal artery renal vein Kidney Anatomy
blood filtration tubular reabsorption and secretion Nephron Functioning “refreshed” blood urine
glomerulus efferent arteriole Bowman’s capsule afferent arteriole proximal convoluted tubule artery distal convoluted tubule peritubular capillaries vein collecting duct loop of Henle
Each kidney contains over 1 million nephrons and thousands of collecting ducts renal cortex renal medulla DCT Glomerulus PCT Collecting duct Loop of Henle
efferent arteriole afferent arteriole Bowman’s capsule glomerulus Glomerular Filtration Filters blood; proteins can’t pass through
Composition of Glomerular Filtrate • Water • Small Soluble Organic Molecules • Mineral Ions
Proximal Convoluted Tubule Reabsorbs: water, glucose, amino acids, and sodium. • 65% of Na+ is reabsorbed • 65% of H2O is reabsorbed • 90% of filtered bicarbonate (HCO3-) • 50% of Cl- and K+
Loop of Henle Creates a gradient of increasing sodium ion concentration towards the end of the loop within the interstitial fluid of the renal pyramid. • 25% Na+ is reabsorbed in the loop • 15% water is reabsorbed in the loop • 40% K is reabsorbed in the loop
Distal Convoluted Tubule Under the influence of the hormone aldosterone, reabsorbs sodium and secretes potassium. Also regulates pH by secreting hydrogen ion when pH of the plasma is low. • only 10% of the filtered NaCl and 20% of water remains
Collecting Duct Allows for the osmotic reabsorption of water. ADH (antidiuretic hormone)- makes collecting ducts more permeable to water-- produce concentrated urine
Urine • Water- 95% • Nitrogenous waste: • urea • uric acid • creatinine • Ions: • sodium • potassium • sulfate • phosphate From the original 1800 g NaCl, only 10 g appears in the urine
heart receptors hypothalamus Hormonal Control of Kidney Function high plasma solute concentration low blood volume
posterior pituitary antidiuretic hormone collecting ducts Hormonal Control of Kidney Function hypothalamus
ureters internal sphincters external sphincters urethra Urinary Bladder
Bladder • Mucosa (transitional epithelium) • Muscular layer (detrusor muscle): 3 layers of smooth muscle • Fibrous adventia
Sphincter Muscles on Bladder • Internal urethral sphincter: • Smooth muscle • Involuntary control • More superiorly located • External Urethral sphincter: • Skeletal muscle • Voluntary control • Posteriorly located
Diuresis (Micturition) When bladder fills with 200 ml of urine, stretch receptors transmit impulses to the CNS and produce a reflex contraction of the bladder (PNS)
Urinalysis • characteristics: • smell- ammonia-like • pH- 4.5-8, ave 6.0 • specific gravity– more than 1.0; ~1.001-1.003 • color- affected by what we eat: salty foods, vitamins
Color Color- pigment is urochrome Yellow color due to metabolic breakdown of hemoglobin (by bile or bile pigments) Beets or rhubarb- might give a urine pink or smoky color Vitamins- vitamin C- bright yellow Infection- cloudy
Specific Gravity Water: s.g. = 1g/liter; Urine: s.g. ~ 1.001 to 1.030 Pyelonephritus- urine has high s.g.; form kidney stones Diabetes insipidus- urine has low s.g.; drinks excessive water; injury or tumor in pituitary
Abnormal Constitutes of Urine • Glucose- when present in urine condition called glycosuria (nonpathological) [glucose not normally found in urine] • Indicative of: • Excessive carbohydrate intake • Stress • Diabetes mellitus
Abnormal Constitutes of Urine Albumin-abnormal in urine; it’s a very large molecule, too large to pass through glomerular membrane > abnormal increase in permeability of membrane Albuminuria- nonpathological conditions- excessive exertion, pregnancy, overabundant protein intake-- leads to physiologic albuminuria Pathological condition- kidney trauma due to blows, heavy metals, bacterial toxin
Abnormal Constitutes of Urine Ketone bodies- normal in urine but in small amts Ketonuria- find during starvation, using fat stores Ketonuria is couples w/a finding of glycosuria-- which is usually diagnosed as diabetes mellitus RBC-hematuria Hemoglobin- Hemoglobinuria- due to fragmentation or hemolysis of RBC; conditions: hemolytic anemia, transfusion reaction, burns or renal disease
Abnormal Constitutes of Urine Bile pigments- Bilirubinuria (bile pigment in urine)- liver pathology such as hepatitis or cirrhosis WBC- Pyuria- urinary tract infection; indicates inflammation of urinary tract Casts- hardened cell fragments, cylindrical, flushed out of urinary tract WBC casts- pyelonephritus RBC casts- glomerulonephritus Fatty casts- renal damage
Urinary Tract Disordersoverall outline • Incontinence & retention • UTI’s • Inflammatory disorders • Nephrotic syndrome • Urinary tract obstruction • Stones • Hydronephrosis • Tumors • Renal cell carcinoma • Bladder cancer • Congenital disorders • Polycystic kidneys • Wilm’s tumor (nephroblastoma) • Renal failure • Acute • Chronic • Dialysis
Urinary Incontinence Loss of voluntary control of bladder Frequently called “neurogenic bladder” Many causes Enuresis = involuntary control after age 4 or 5 Types: Stress Urge Overflow Urinary retention Called “residual urine” Causes : Anatomical defects Neurogenic defects Treated with “catheterization” Incontinence, retention, & catheters
Urinary Tract Infections Urethritis; Cystitis; Pyelonephritis • Etiology • Ascending infection ----- women > men • Prostatic hypertrophy with urinary retention • Incomplete emptying of bladder with urinary stasis • Blood borne pathogens • Pathophysiology of UTI’s • Dysuria, urgency, & nocturia • Systemically get fever & malaise • CVA tenderness in pyelonephritis
Glomerulonephritis Acute proteinuria, edema, oliguria Chronic autoimmune disease Can lead to irreversible kidney damage Inflammatory disorders(1) glomerulonephritis (2) nephrotic syndrome
Nephrotic Syndrome • Glomerular disorder where one loses the capacity to retain protein, especially albumin • Symptoms • severe edema (anasarca) • * can get skin breakdown since impaired arterial flow • proteinuria • hypoalbuminemia • oliguria • Etiol: • Toxic agents (lead, mercury) • Toxic drugs (aminoglycosides) • Diseases (diabetes, lupus • Key = any significant problem with the • glomerulus can lead • to nephrotic syndrome
Tumors Note that primary symptom = hematuria Renal Cell Ca = most common, unilateral, adeno Ca from tubular epithelium See picture Bladder Ca = usually from transitional epithelium Neurogenic bladder Renal Calculi (kidney stones) Causes: Calcium, Uric acid, Urine crystals Symptoms: renal colic, N&V, chills, fever Risk factors: prolong dehydration, prolong immobilization, infection Treatment: surgery,lithotripsy Anomalies Strictures Kinks Ptosis Pelvic kidney Obstructive Disorders
These result in: • Hydronephrosis • Hydroureter • If these conditions exist longer than 2 months get destruction of kidney Major sites of urinary tract obstruction
Congenital Diseases • Vesicoureteral reflux • Due to ectopic insertion of ureter into bladder. If far away from trigone, do not get adequate compression of ureter when voiding & get reflux • Incidence: 1/1000 • If one gets it each sibling(to be) has 50% incidence • Girls> boys; 10:1 ratio • Ectopic kidney • May get kinking of ureter • Usually in pelvis • Asymptomatic • Renal agenesis • Usually unilateral & left kidney • 2 types: (1) occurs randomly (2) genetic • Asymptomatic • Remaining kidney becomes large since compensatory hypertrophy
Congenital Diseases (cont) • Polycystic kidney (2 types • In adults (see picture) • Genetic etiol ----- autosomal dominant • Clinically seen in adults • Between age 30 – 40 one begins to get renal failure • Transplant for treatment • In children • Genetic etiol --- autosomal recessive • Manifest at birth; usually fatal or infant stillborn • Rare • Wilm’s tumor (nephroblastoma) • Most common tumor of children; usually unilateral
Acute renal failure Abrupt decrease in renal function Nitrogenous wastes accumulate Usually reversible Symptoms Oliguria Drowsiness Altered levels of consciousness Causes Glomerular disease Severe pyelonephritis Nephrotoxins that damages tubular epithelium Ischemic causes shock ATN (acute tubular necrosis) e.g. burns(hgb accumulates) e.g. trauma (myoglobin accumulates) Renal Failure