Download

1 / 28
290 likes | 298 Views
1-line Treatment of Advanced-NSCLC WT. Cesare Gridelli Division of Medical Oncology “S.G. Moscati” Hospital – Avellino (Italy) cgridelli@libero.it. First-Line Treatment of A-NSCLC in EU. EGFR mutation (del 19 or L858R in exon 21). EGFR-TKI. Radiotherapy CNS Central airways Bone

E N D
1-line Treatment of Advanced-NSCLC WT Cesare Gridelli Division of Medical Oncology“S.G. Moscati” Hospital – Avellino (Italy)cgridelli@libero.it
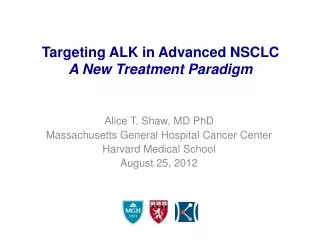
First-Line Treatment of A-NSCLC in EU EGFR mutation (del 19 or L858R in exon 21) EGFR-TKI • Radiotherapy • CNS • Central airways • Bone • Soft tissue • Platinum plus • Pemetrexed or gemcitabine or taxanes or vinorelbine • OR • Platinum combination plus • Bevacizumab* (PS 0,1) • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) EGFR-mutation analysis EGFR wild type (or not done) Non-squamous cell carcinoma Metastatic NSCLC, PS 0-2 • Platinum plus • Gemcitabine or taxane or vinorelbine • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) Squamous cell carcinoma 3 2 1 2
First-Line Treatment of Advanced NSCLCNCCN Guidelines EGFR mutation and ALK negative Doublet chemotherapy (category 1) OR Bevacizumab + chemotherapy (if criteria met) OR Cisplatin/pemetrexed (category 1) (if criteria met) OR Cetuximab/vinorelbine/cisplatin(category 2B) • Adenocarcinoma • Large cells • NSCLC NOS EGFR mutation positive Erlotinib PS 0-1 ALK positive Crizotinib Doublet chemotherapy (category 1) OR Cetuximab/vinorelbine/ cisplatin (category 2B) PS 2 Chemotherapy PS 0-1 PS 3-4 Best supportive care only Squamous cell carcinoma PS 2 Chemotherapy PS 3-4 Best supportive care
First-Line Treatment of Advanced NSCLC EGFR mutation (del 19 or L858R in exon 21) EGFR-TKI • Radiotherapy • CNS • Central airways • Bone • Soft tissue • Platinum plus • Pemetrexed or gemcitabine or taxanes or vinorelbine • OR • Platinum combination plus • Bevacizumab PS 0,1) • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) EGFR-mutation analysis EGFR wild type (or not done) Non-squamous cell carcinoma Metastatic NSCLC, PS 0-2 • Platinum plus • Gemcitabine or taxane or vinorelbine • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) Squamous cell carcinoma
First-Line Treatment of Advanced NSCLC EGFR mutation (del 19 or L858R in exon 21) EGFR-TKI • Radiotherapy • CNS • Central airways • Bone • Soft tissue • Platinum plus • Pemetrexed or gemcitabine or taxanes or vinorelbine • OR • Platinum combination plus • Bevacizumab PS 0,1) • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) EGFR-mutation analysis EGFR wild type (or not done) Non-squamous cell carcinoma Metastatic NSCLC, PS 0-2 • Platinum plus • Gemcitabine or taxane or vinorelbine • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) Squamous cell carcinoma
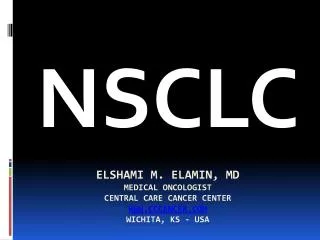
100 Hazard ratio, 0.79; P=0.003 80 BPC group(305 events in 417 patients) 60 Overall Survival, % 40 PC group(344 events in 433 patients) 20 0 0 6 12 18 24 30 36 42 Month BPC, bevacizumab-paclitaxel-carboplatin; PC, paclitaxel-carboplatin.The median survival was 12.3 months in the group assigned to chemotherapy plus bevacizumab versus 10.3 months in the chemotherapy-alone group.Sandler A, et al. N Engl J Med. 2006;355(24):2542-2550.
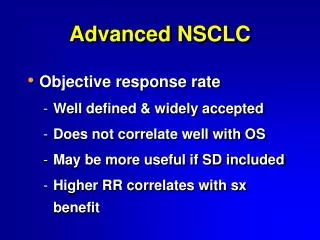
Avastin-based therapy (n=602) extends OS to 14.2 months 31% reduction in the risk of death (HR=0.69) 0.8 0.6 0.4 0.2 0 Avastin + CP (n=300) CP (n=302) Probability of OS 10.3 14.2 0 6 12 18 24 30 36 42 48 Duration of OS (months)
First-Line Treatment of Advanced NSCLCESMO Guidelines EGFR mutation (del 19 or L858R in exon 21) EGFR-TKI • Radiotherapy • CNS • Central airways • Bone • Soft tissue • Platinum plus • Pemetrexed or gemcitabine or taxanes or vinorelbine • OR • Platinum combination plus • Bevacizumab PS 0,1) • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) EGFR-mutation analysis EGFR wild type (or not done) Non-squamous cell carcinoma Metastatic NSCLC, PS 0-2 • Platinum plus • Gemcitabine or taxane or vinorelbine • Elderly/PS 2 • Platinum combination (preferred in fit elderly) or • Monotherapy (preferred in unfit elderly) Squamous cell carcinoma
Cisplatin With Pemetrexed or GemcitabineJMDB Trial 1.0 1.0 1.0 1.0 0.8 0.8 0.8 0.8 0.6 0.6 0.6 0.6 0.4 0.4 0.4 0.4 0.2 0.2 0.2 0.2 0.0 0.0 0.0 0.0 0 0 0 0 6 6 6 6 12 12 12 12 18 18 18 18 24 24 24 24 30 30 30 30 Median; 95% CI Median; 95% CI CP 11.8; 10.4, 13.2 CP 5.3; 4.8, 5.7 CG 10.4; 9.6, 11.2 CG 4.7; 4.4, 5.4 CP vs CG Adjusted HR; 95% CI 0.81; 0.70, 0.94 CP vs CG Adjusted HR; 95% CI 0.90; 0.79, 1.02 PFS Probability Survival Probability Survival Time (months) in PatientsWith Non-squamous Histology PFS (months) in Patients With Non-squamous Histology Median; 95% CI Median; 95% CI CP 9.4; 8.4, 10.2 CP 4.4; 4.1, 4.9 CG 10.8; 9.5, 12.1 CG 5.5; 4.6, 5.9 PFS Probability Survival Probability CP vs CG Adjusted HR; 95% CI 1.23; 1.00, 1.51 CP vs CG Adjusted HR; 95% CI 1.36; 1.12, 1.65 Survival Time (months) in Patients With Squamous Cell Carcinoma PFS (months) in Patients With Squamous Cell Carcinoma Cisplatin/pemetrexed provides similar efficacy with better tolerability and more convenient administration than cisplatin/gemcitabine in NSCLC CP, cisplatin-pemetrexed.Scagliotti GV, et al. J Clin Oncol. 2008;26(21):3543-3551.
Maintenance TherapyContinuation vs Switch ‘Continuation’ maintenance with TT(eg, bevacizumab) Selection of patients with a better prognosis ‘Continuation’ maintenance with the chemo drug X P + X± TT × 4 cycles Stabilisation or objective response 50% ‘Switch’ maintenance with a new drug TT (EGFR TKI for SD patients) QoLSymptom controlToxicities ‘Switch’ maintenance with a new chemo drug
SATURN: Sequential Tarceva in unresectable NSCLC Stage IIIb/IV NSCLC 4 cycles of a first-line standard platinum-based doublet Planned Recruitment = 1,700 Tumour samples (mandatory) Screening Period TITAN No progression (n=899) Progression EGFR protein expression (IHC) results Randomisation with stratification Study Period Erlotinib 150mg/day Placebo Until PD, death or unacceptable toxicity Until PD, death or unacceptable toxicity
OS from randomization in all patients 1.0 0.8 0.6 0.4 0.2 0 HR=0.81 (0.70–0.95) Log-rank p=0.0088 Erlotinib (n=438) Placebo (n=451) OS probability 11.0 12.0 0 3 6 9 12 15 18 21 24 27 30 33 36 Time (months) *OS is measured from time of randomisation into the maintenance phase;ITT = intent-to-treat population Cappuzzo et al,WCLC 2009
OS according to response to first-line chemo SD CR/PR 1.0 0.8 0.6 0.4 0.2 0 1.0 0.8 0.6 0.4 0.2 0 HR=0.94 (0.74–1.20) HR=0.72 (0.59–0.89) Log-rank p=0.0019 Log-rank p=0.6181 OS probability 9.6 11.9 12.0 12.5 0 3 6 9 12 15 18 21 24 27 30 33 36 0 3 6 9 12 15 18 21 24 27 30 33 36 Time (months) Time (months) Multivariate HR for OS in SD population 0.71, p=0.0019 Measured from time of randomisation into the maintenance phase
PARAMOUNT: Study Design Study Treatment Period Induction Therapy (4 cycles) 21 to 42 Days Maintenance Therapy (Until PD) Progression 500 mg/m2 Pemetrexed + BSC, d1, q21d • Patients enrolled if: • Nonsquamous NSCLC • No prior systemic treatment for lung cancer • ECOG PS 0/1 CR, PR, SD 2:1 Randomization Placebo + BSC, d1, q21d • Stratified for: • PS (0 vs 1) • Disease stage (IIIB vs IV) prior to induction • Response to induction (CR/PR vs SD) 500 mg/m2 Pemetrexed +75 mg/m2 Cisplatin, d1, q21d PD
PARAMOUNT: Investigator Assessed PFS (from Maintenance) Pem + BSC Placebo + BSC Pemetrexed: median =4.1 mos (3.2-4.6) Placebo: median =2.8 mos (2.6-3.1) Log-rank P=0.00006 Unadjusted HR: 0.62 (0.49-0.79)
PARAMOUNT: Final OS from Randomization 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 Survival Probability Log-rank P = 0.0195 Unadjusted HR: 0.78 (95% CI: 0.64–0.96) 0 3 6 9 12 15 18 21 24 27 30 33 36 Time from Randomization (Months) Patients at Risk Pem + BSC359 333 272 235 200 166 138 105 79 43 15 2 0 Placebo + BSC 180 169 131 103 78 65 49 35 23 12 8 3 0
PARAMOUNT: Final OS from Induction Pemetrexed Median OS =16.9 mos (95% CI: 15.8–19.0) Placebo Median OS =14.0 mos (95% CI: 12.9–15.5) Log-rank P=0.0191 HR=0.78 (95% CI: 0.64–0.96) 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 Survival Probability 0 3 6 9 12 15 18 21 24 27 30 33 36 Time from Induction (Months) Patients at Risk Pem + BSC 359 335 276 234 200 164 138 106 77 42 15 2 0 Placebo + BSC 180 168 132 103 78 63 49 35 23 12 8 3 0
1.0 CR/PRHR=0.81 (0.59–1.11) Pemetrexed + BSCMedian OS=16.9 months (95% CI, 15.8–19.0) 0.8 0.6 1.0 Placebo + BSCMedian OS=14.0 months (95% CI, 12.9–15.5) 0.4 0.2 0.8 0.0 Survival Probability 0.6 0 3 6 9 12 15 18 21 24 27 30 33 36 Survival Probability 1.0 0.4 Stable DiseaseHR=0.76 (0.57–1.01) 0.8 0.2 HR=0.78 (95% CI, 0.64–0.96) Log-rank P=0.0191 0.6 0.4 0.0 0.2 0 3 6 9 12 15 18 21 24 27 30 33 36 Time From Induction, months 0.0 0 3 6 9 12 15 18 21 24 27 30 33 36 Time From Randomisation, months
Mean value at baseline (Cycle 0) ∆ Mean change from baseline EQ-5D UK population-based index score EQ-5D VAS * * ∆3.01 ∆5.99 * ∆6.15 ∆4.90 ∆0.03 ∆0.02 ∆1.55 ∆0.69 ∆1.42 ∆1.82 ∆-0.02 ∆-0.01 ∆5.76 ∆0.01 ∆0.04 ∆0.00 ∆1.65 ∆3.15 Improvement Mean Score (Scale -0.59 to +1.00) Improvement Mean Rating (Scale 0 to 100) ∆0.00 ∆0.01 ∆1.24 ∆0.01 ∆0.01 ∆0.01 N=265 132 241 129 160 83 149 66 108 48 98 36 N=266 126 239 127 162 81 147 65 107 48 98 36 Maintenance Cycles Maintenance Cycles EQ-5D, EuroQol 5-dimensional questionnaire; VAS, visual analog scale.*P≤0.05, comparing the difference in mean changes from baseline between treatment arms.Gridelli C, et al. J Thorac Oncol. 2012;7(11):1713-1721.
Change in ECOG Performance Status from Baseline to Last Maintenance Treatment 12.4% 16.0% 76.2% 78.6% 7.8% 9.0%
PARAMOUNT: Long Term Safety * 10 cycles = 10 total cycles (4 induction cycles + 6 maintenance cycles) † Although incidence of G 3-4 neutropenia higher with long-term use; this did not translate into increased G 3-4 infections.
J Thorac Oncol, in press Palliative radiation during pemetrexed plus cisplatin first-line treatment for advanced non-small cell lung cancer (NSCLC): Patient safety in the JMDB and PARAMOUNT trials 1Giorgio V Scagliotti, 2Cesare Gridelli, 3Filippo de Marinis, 4Bonne Biesma, 5Martin Reck, 6Belen San Antonio, 7Annamaria Hayden Zimmermann, 8Carla Visseren-Grul, 9Nadia Chouaki, 10Luis Paz-Ares 1University of Torino, San Luigi Hospital, Orbassano (Torino), Italy; 2San Giuseppe Moscati Hospital, Avellino, Italy; 3San Camillo - Forlanini Hospital, Rome, Italy; 4Jeroen Bosch Hospital, Hertogenbosch, Netherlands; 5Hospital Grosshansdorf, Grosshansdorf, Germany; 6Eli Lilly and Company, Madrid, Spain; 7Eli Lilly and Company, Indianapolis, IN, USA; 8Eli Lilly and Company, Houten, Netherlands; 9Eli Lilly and Company, Paris, France; 10Seville University Hospital, Seville, Spain
Possibly drug-related adverse events during palliative XRT or within 2 weeks after the end of the last fraction in JMDB and PARAMOUNT (N=65) *In JMDB two patients experienced AEs; 1 Grade 2 (Gr 2) anemia and 1 Gr 2 radiation dermatitis. *In Paramount 10 patients experienced AEs during the induction phase of treatment Other events commonly associated with the administration of chemotherapy and XRT, such as lung toxicities (e.g. pneumonitis) and esophagitis, were not reported. • Dose range for 12 patients with AEs 8-34 Gy • Half of patients with adverse events received palliative radiation within 7 days of the last chemotherapy • Of the patients with brain metastases (n=5) none reported adverse events related to palliative XRT