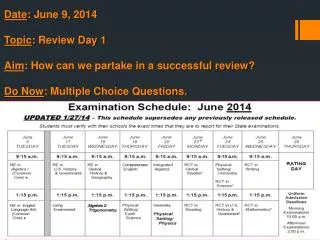
Download
1 / 15
160 likes | 351 Views
TOPSoccer Round Table Discussion Atlantoaxial Instability (AAI) Region IV TOPSoccer Symposium April 2010. “And the answer is?”. Atlantoaxial Instability (AAI). What is Atlantoaxial Instability or AAI?

E N D
TOPSoccer Round Table DiscussionAtlantoaxial Instability (AAI)Region IV TOPSoccer SymposiumApril 2010 “And the answer is?” 1
Atlantoaxial Instability (AAI) What is Atlantoaxial Instability or AAI? Atlantoaxial instability (AAI) is a common orthopedic problem seen in people with Down syndrome. Although it has a complicated name and sounds somewhat intimidating, for the most part it causes no problems to those who have it. In order to understand AAI, it is important to understand a little about the function and structure of the spinal cord, nerves, vertebrae and ligaments. Sources for following information: American Academy of Pediatrics, Committee on Sports Medicine. Atlantoaxial instability in Down syndrome. Pediatrics. Vol. 107 No. 2, February 2001, pp. 442-449 [/] 2
Atlantoaxial Instability (AAI) Vertebrae are irregularly shaped bones organized in to a column in the back of the body that runs from the base of the brain to the pelvis. The spinal cord runs through and is protected by this stack of vertebrae. There are 33 vertebrae, which are generally broken in to four regions: cervical (7), thoracic (12), lumbar (5) and the vertebra of the pelvis. Cervical vertebrae are located in the neck region and are abbreviated as C1-C7. If you bend your head forward and run your fingers down the back of your head, the first large bump that you feel is your C1 or cervical-1 vertebra. The next one down is C2 and so forth. C1 is referred to as the atlas vertebra and C2 as the axis vertebra. Misalignment between these vertebrae is referred to as atlantoaxial instability or AAI. 3
Atlantoaxial Instability (AAI) Vertebrae are held in place by muscles and ligaments. The functions of the vertebral column include protection of the spinal cord and internal organs, structural support for the head and maintaining both flexibility and mobility. Since people with Down syndrome have low muscle tone and lax ligaments, their vertebrae can become misaligned. When the C1 and the C2 vertebrae are misaligned, you have AAI 4
Atlantoaxial Instability (AAI) Diagnosis of AAI Most cases of asymptomatic AAI are made through screening x-rays. All children with Down syndrome should be screened for AAI by the age of 3 (AAP recommendation). The diagnosis of symptomatic AAI is usually made either through neurological exam (physical exam that examines how the nerves are working) and/or by x-ray. 5
Atlantoaxial Instability (AAI) Types of AAI There are two types of atlantoaxial instability - asymptomatic AAI and symptomatic AAI. Asymptomatic AAI means that AAI can be seen on an x-ray, but it is not causing any neurologic problems in the person who has it. Symptomatic AAI means that AAI is present on an x-ray, and it is causing some neurologic problems for the person that has it. Symptomatic AAI is of concern. Somewhere between 10% to 20% of people with Down syndrome have asymptomatic AAI on x-ray, and only 1% to 2% of people with Down syndrome have symptomatic AAI. 6
Atlantoaxial Instability (AAI) Neurologic Manifestations of Symptomatic AAI One of the jobs of the vertebral column is to protect the spinal cord, which runs inside it. The spinal cord is a collection of nerves that is protected by the vertebral column. Symptomatic AAI causes a variety of different neurologic symptoms such as: • Clumsiness • Lack of Coordination • Difficulty walking • Walking with an abnormal gait (e.g. limping) • Getting tired easily • Nerve pain or limited ability to move the neck • Spasticity - tightness in the muscles • Clonus - muscle contractions or spasms 7
Atlantoaxial Instability (AAI) So, What Are We To Do? The Academy of Pediatrics (AAP) in 1984 issued the position statement that all children with Down Syndrome who wish to participate in sports should have cervical spine X-rays. Those who show a distance of more than 4.5 mm, restrictions on sports is advised. AAP released a revised statement in July of 1995 which retired the above1984 statement when the Committee on Sports Medicine decided that uncertainty exists concerning the value of X-rays in screening for possible catastrophic neck injury in athletes with Down Syndrome. 8
Atlantoaxial Instability (AAI) Treatment of AAI • Asymptomatic AAI does not require any treatment. Most often parents are simply advised what symptoms to watch for in the person with AAI. • If a person is showing signs of spinal cord compression, treatment is indicated. The goals of treating symptomatic AAI is to protect the spinal cord, stabilize the spinal column or vertebrae and decompress any trapped nerves. Depending on the extent of the problem, spinal cord stabilization can be achieved through wearing a soft collar, halter traction with pain medication and muscle relaxants and possibly surgery. 9
Atlantoaxial Instability (AAI) The Difficulty Factor • AAI can be found in people with rheumatoid arthritis • Individuals with various forms of dwarfism have AAI • AAI can be the result of extreme bad posture • There are over 400,000 Down Syndrome people in the United States • 40,000 to 80,000 could have asymptomatic AAI • 4,000 to 8,000 could have symptomatic AAI • Statistics provided by the Mile High Down Syndrome Association showed 6 catastrophic injuries were reported since 1984 • One case involved a patient having neck pain and then gradual paralysis after playing soccer (with no known injury during play) 10
Atlantoaxial Instability (AAI) Things to Remember • We are NOT doctors; Parental concerns should be directed towards the player’s physician • If we see a difference in a players ability from season to season that might be related to one of the symptoms mentioned previously, advise the parents and document on the player information sheet • Control practices and games (a requirement for all US Youth Soccer participants) • Be aware but don’t be afraid – common sense prevails 11
Atlantoaxial Instability (AAI) Instill game control within your practices and games • Prevent collisions between players, buddies and coaches • Do not allow players, buddies or coaches to “hard kick” the ball • Throw-ins should be discouraged while other players are present • Warm-ups should include exercises that limit pressure to the neck area for those Down Syndrome players • If the parent asks if their player should be X-rayed, that question should be directed towards the players doctor Mac Macsovits Executive Director Mile High Down Syndrome Association macm@mhdsa.org 303-756-6069 12
Atlantoaxial Instability (AAI) Parent Participation Parents have an obligation to advise those working with their players of any medical restrictions • Get it in writing with the parent’s signature • League Registration Form & Player Information Sheet • Retain these forms following your Club/Leagues Record Retention Policy • At a minimum, if the player has symptomatic AAI, require a doctor’s release • Register all players to ensure medical and liability coverage 13
Atlantoaxial Instability (AAI) OPEN DISCUSSION 14
Colorado Youth SoccerAtlantoaxial Instability (AAI)TOPSoccer SymposiumApril 2010Questions? 15