Download
1 / 19
190 likes | 340 Views
Potential Sources of Racial and Ethnic Healthcare Disparities – Healthcare Systems-level Factors. Cultural and linguistic barriers – many non-English speaking patients report having difficulty accessing appropriate translation services

E N D
Potential Sources of Racial and Ethnic Healthcare Disparities – Healthcare Systems-level Factors • Cultural and linguistic barriers – many non-English speaking patients report having difficulty accessing appropriate translation services • Lack of stable relationships with primary care providers – minority patients, even when insured at the same level as whites, are more likely to receive care in emergency rooms and have less access to private physicians • Financial incentives to limit services – may disproportionately and negatively affect minorities • “Fragmentation” of healthcare financing and delivery
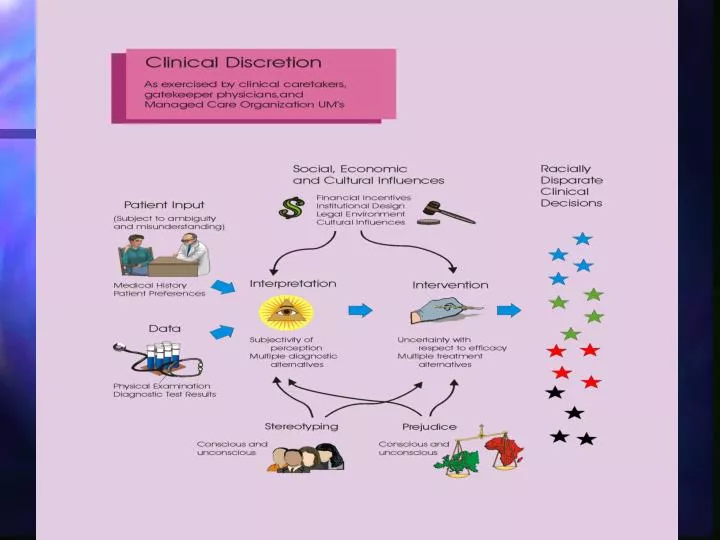
Disparities in the Clinical Encounter: The Core Paradox How could well-meaning and highly educated health professionals, working in their usual circumstances with diverse populations of patients, create a pattern of care that appears to be discriminatory?
Disparities in the Clinical Encounter: The Core Paradox Possibilities examined: bias (prejudice), uncertainty, stereotyping • Bias – no evidence suggests that providers are more likely than the general public to express biases, but some evidence suggests that unconscious biases may exist • Uncertainty – a plausible hypothesis, particularly when providers treat patients that are dissimilar in cultural or linguistic background • Stereotyping – evidence suggests that physicians, like everyone else, use these ‘cognitive shortcuts’
Stereotyping: A Definition Stereotyping can be defined as the process by which people use social categories (e.g. race, sex) in acquiring, processing, and recalling information about others. Stereotyping beliefs may serve important functions - organizing and simplifying complex situations and giving people greater confidence in their ability to understand, predict, and potentially control situations and people.
Stereotyping: Risks Can exert powerful effects on thinking and actions at an implicit, unconscious level, even among well-meaning, well-educated persons who are not overtly biased. Can influence how information is processed and recalled. Can exert “self-fulfilling” effects, as patients’ behavior may be affected by providers’ overt or subtle attitudes and behaviors.
Stereotyping: When Is It in Action? Situations characterized by time pressure, resource constraints, and high cognitive demand promote stereotyping due to the need for cognitive ‘shortcuts’ and lack of full information.
What is the Evidence that Physician Biases and Stereotypes May Influence the Clinical Encounter? • van Ryn and Burke (2000) - study conducted in actual clinical settings found that doctors are more likely to ascribe negative racial stereotypes to their minority patients. These stereotypes were ascribed to patients even when differences in minority and non-minority patients’ education, income, and personality characteristics were considered. • Finucane and Carrese (1990) - Physicians more likely to make negative comments when discussing minority patients’ cases.
What is the Evidence that Physician Biases and Stereotypes may Influence the Clinical Encounter (cont’d)? • Rathore et al. (2000) – found that medical students were more likely to evaluate a white male “patient” with symptoms of cardiac disease as having “definite” or “probable” angina, relative to a black female “patient” with objectively similar symptoms. Abreu (1999) – found that mental health professionals and trainees were more likely to evaluate a hypothetical patient more negatively after being “primed” with words associated with African American stereotypes.
“Patients” experiencing symptoms of heart disease, from Schulman et al. (1999)
“Patients” experiencing symptoms of heart disease, from Schulman et al. (1999)
SUMMARY OF FINDINGS Racial and ethnic disparities in health care exist and, because they are associated with worse outcomes in many cases, are unacceptable. Racial and ethnic disparities in health care occur in the context of broader historic and contemporary social and economic inequality, and evidence of persistent racial and ethnic discrimination in many sectors of American life. Many sources – including health systems, health care providers, patients, and utilization managers – contribute to racial and ethnic disparities in health care.
SUMMARY OF FINDINGS (Continued) Bias, stereotyping, prejudice, and clinical uncertainty on the part of healthcare providers may contribute to racial and ethnic disparities in healthcare. While indirect evidence from several lines of research supports this statement, a greater understanding of the prevalence and influence of these processes is needed and should be sought through research. Racial and ethnic minority patients are more likely than white patients to refuse treatment, but differences in refusal rates are generally small, and minority patient refusal does not fully explain healthcare disparities.
SUMMARY OF RECOMMENDATIONS GENERAL RECOMMENDATIONS Increase awareness of racial and ethnic disparities in health care among the general public and key stakeholders, and increase health care providers’ awareness of disparities. LEGAL, REGULATORY, AND POLICY RECOMMENDATIONS Avoid fragmentation of health plans along socioeconomic lines, and take measures to strengthen the stability of patient-provider relationships in publicly funded health plans;
LEGAL, REGULATORY, AND POLICY RECOMMENDATIONS (Continued) Increase in the proportion of underrepresented U.S. racial and ethnic minorities among health professionals; Apply the same managed care protections to publicly funded HMO enrollees that apply to private HMO enrollees; Provide greater resources to the U.S. DHHS Office of Civil Rights to enforce civil rights laws.
HEALTH SYSTEMS INTERVENTIONS Promote the consistency and equity of care through the use of evidence-based guidelines; Structure payment systems to ensure an adequate supply of services to minority patients, and limit provider incentives that may promote disparities; Enhance patient-provider communication and trust by providing financial incentives for practices that reduce barriers and encourage evidence-based practice; Promote the use of interpretation services where community need exists. The use of community health workers and multidisciplinary treatment and preventive care teams should also be supported.
EDUCATION Patient education programs should be implemented to increase patients’ knowledge of how to best access care and participate in treatment decisions. Integrate cross-cultural education into the training of all current and future health professionals.
DATA COLLECTION AND MONITORING Collect and report data on health care access and utilization by patients’ race, ethnicity, socioeconomic status, and where possible, primary language; Include measures of racial and ethnic disparities in performance measurement; Monitor progress toward the elimination of health care disparities; Report racial and ethnic data by OMB categories, but use subpopulation groups where possible.
NEEDED RESEARCH Conduct further research to identify sources of racial and ethnic disparities and assess promising intervention strategies, and; Conduct research on ethical issues and other barriers to eliminating disparities.