Download
1 / 27
290 likes | 1.37k Views
The Have and Have Nots of Healthcare. Economic segregation in healthcare the District of Columbia example. Gloria WilderBrathwaite, MD, MPH. July 2004, Washington post: Income inequality In DC is wider than In any major US city.

E N D
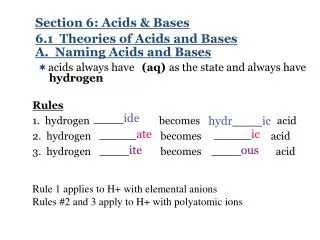
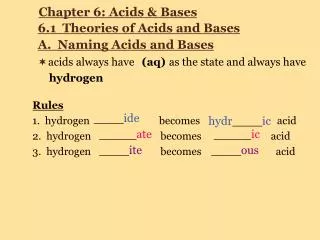
The Have and Have Nots of Healthcare Economic segregation in healthcare the District of Columbia example. Gloria WilderBrathwaite, MD, MPH
July 2004, Washington post: Income inequality In DC is wider than In any major US city. The wealthiest 5th percent of DC residents (average income 186,000). Make more than 31 times the poorest 5th percent (average income 6,126). Over the last two decades the top 5th percentile of residents of DC have seen their income rise 38% while the bottom 5th have enjoyed only a 3% adjustment in household income. The Poverty Link
What Is the Significance of the Income Gap? • Creates two cultural groups: The have’s and have nots. • Elite class vs. Impoverished class. • Disappearing privileged class (middle class).
What Is Poverty? • Federal poverty level family of three in 2004 is $15,670. • If you make less than this you qualify for public assistance, Medicaid, food stamps, temporary assistance to needy families (welfare), housing and daycare subsidy. • A family of three receiving welfare gets $8,112 per year ($676 per month). About one half of the poverty level. • Even after getting public assistance this group remains well below the poverty level. • This group is not legally permitted to work to subsidize this income. Is this fair opportunity?
2 0 0 1 2 2 0 0 1 5 2 0 0 1 1 2 0 0 1 6 2 0 0 1 7 2 0 0 0 8 2 0 0 1 0 2 0 0 1 8 2 0 0 0 9 2 0 0 0 7 2 0 0 0 1 2 0 0 0 5 2 0 0 0 2 2 0 0 3 7 2 0 0 1 9 2 0 0 0 3 2 0 0 2 4 P e r c e n t I n c o m e < $ 1 5 , 0 0 0 2 0 0 2 0 0 . 0 4 - 0 . 0 7 0 . 0 7 - 0 . 1 6 2 0 0 3 2 0 . 1 6 - 0 . 3 1 Where Is Poverty in DC? Distribution of Poverty by Zip
Percent of residents below 200% of the federal poverty level by zip code, 2000 DC Primary Care Association
Percent of adults without health insurance, 2001-2002 DC Primary Care Association
Percent of adults with no regular source of care,2001-2002 “Regular source of care” includes doctors’ offices, health centers, and outpatient hospital departments. DC Primary Care Association
Adult chronic disease burden, 2001-2002 Includes asthma, diabetes and hypertension. DC Primary Care Association
Avoidable hospitalization rates among kids 0-17, 2000-2003 DC Primary Care Association
Avoidable hospitalizations among adults 18-39, 2000-2003 DC Primary Care Association
Community health centers by type, 2004 • General primary care = 29 • Homeless shelters = 9 • Pediatrics = 6 • School-based health centers = 3 • Mobile Vans = 5 DC Primary Care Association
Size of health centers (# of patients) and pct of pop below 200% of FPL • More/bigger centers in the central part of the city • Fewer/smaller centers in other parts of the city – Northeast and East of the Anacostia River DC Primary Care Association
Location of Doctors’ Offices by Ward and Quadrant, 2003 Ward # of establishments 1 30 2 252 3 126 4 59 5 131 6 38 7 10 8 29 675 DC Primary Care Association
So What Do We Know About the Effects of Poverty on Healthcare Delivery in DC? • Poor people seem to be clustered in specific zip codes within the city. • These areas have the fewest safety net healthcare providers. • These areas have the highest chronic disease burden and highest admission rates. • The highest proportion of the cities children live within these poverty clusters. • What happens when children are raised in isolated poverty?
Statistics on Children in Poverty DC 2004 • About 130,000 children under 21 live in DC. One third of these children live in poverty (more than any other state in the union). 16% live in extreme poverty (less than 50% of the poverty level). • 60,000 children live with adults who are not their parents. • 53% of 8th graders score below basic in reading, 71% in math. • Only 10% of children living here in the wealthiest and most powerful capitol in the world read on a proficient level.
Who are the uninsured? • There are 45 million uninsured people in the United States. • Two thirds of the uninsured in this country make less than 200% of poverty for a family of four that is $37,620 per year. • In 2003, over 8 in 10 uninsured came from working families-70% from families with one or more full time workers.
Why Advocate? Ethical care doctrine: Is it ok to prescribe treatments that you know the patient cannot comply with?
Why Advocate? Nonmalifience: Do no harm. When does healthcare become harmful?
Why Advocate? Beneficence: Do Good. The higher calling of health care professionals to use their influence for the greater good.
What should we do? • Support expanded primary care and preventive healthcare services in health professional shortage areas. 300,000 DC residents live in primary care shortage areas. • Build less trauma centers and more medical homes. • Reimburse primary care at a fair market rate to end the economically segregated healthcare system. Currently primary care reimbursement is 50% of true cost.
What should we do? • Provide small business loans to doctors wanting to start practices in shortage areas. • Advocate for universal healthcare coverage. Insurance alone is not enough but it is the first step to ending economic inequality in healthcare. • Access is the final step. No more public health only for the poor. All healthcare should be everyone’s healthcare. • The provider of healthcare should be blinded to the payer.
Acknowledgement • DC Primary Care Association • Nicole Lurie, MD , Rand Corporation • Alice Rivilin and Margaret Ross, Brookings Institution • Bureau of Epidemiology and Health Risk Assessment, DC Department of Health