Download
1 / 23
480 likes | 1.45k Views
Off Pump Coronary Artery Bypass Grafting (OPCAB). Off pump surgery is not new. 1964 - IMA as a graft Kolesov Thoracotomy no CPB 1985 - Complete CABG Benetti no CPB 1995 - Minimally Invasive CABG Calafiore

E N D
Off pump surgery is not new 1964 - IMA as a graft Kolesov Thoracotomy no CPB 1985 - Complete CABG Benetti no CPB 1995 - Minimally Invasive CABG Calafiore no CPB Subramanian 1996 - First use of suction Borst Stabilization device Grunderman 1997 - Multivessel suction Jansen Stabilization Device
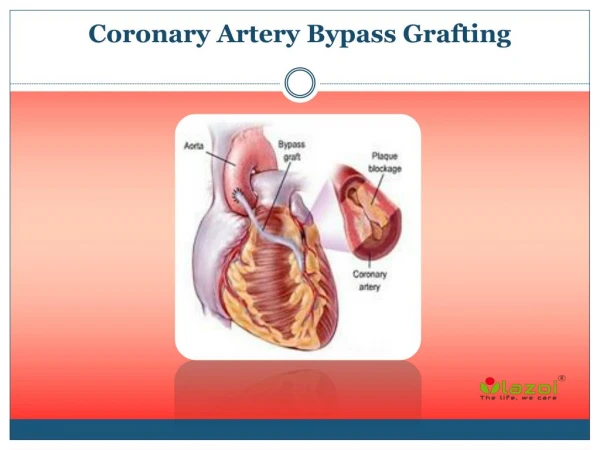
CABG / OPCAB Sternotomy Cardiopulmonary Bypass (CPB) Hypothermia Aortic Cross Clamp Cardiopegia Anastomosis Hemostasis
OPCAB Demands Exposure of post, Lat wall of the heart. Stabilization of target area. Visualization Occlusion of the Coronary Ar. or Shunt. Stable Hemodynamics.
Relative Contraindications • Intramyocardial Coronary Ar. • Very small arteries ( <1m”m). • Calcified arteries. • Poor conduits. • Huge hearts. • Hemodynamic Instability/Ischemia. • Cardiogenic shock.
Pump Morbidity Manipulation Haematologic coagulation Inflammatory of Aorta disorders Response WBC , Hg Bleeding post pump Neurologic dysfunction PLT , IgG syndrome Stroke Reopen Prolonged Ventilation Immunitiy Transfusion Fever Sepsis M Prolonged ICU + Hospital stay M Cost Effectiveness
Pump Benefits - Easy quick Meticulous anastomosis Best choice of Anastomotic site. Possibility of Ar. Reconstruction. - Multiple grafts. - Unloading of Ischemic or failing Heart. - Less stress on the Surgeon (anesthetist).
Problems -Difficult surgery -Haemodynamic disturbances (Organ insults) - Inability to perform complete re-vascularization - Patency rate Solutions Experienced surgeon Experienced and very aware Anesthetist Hybrid procedure (PCI +OPCAB) Do as best as you can. OPCAB Obstacles
OPCAB Benefit - Reduction of: - neurologic complications. - cognitive disorders. - stroke. - Reduction of ventilation time and pulmonary complications - Reduction of blood loss Less transfusions. - Possible less inflammation ? - Shorter I.C.U stay. - Possible earlier discharge? most OPCABG patients are old and with sev. comorbidities.
Neurological Outcome Mechanism of Neurocognitive Disorders in Heart Surgery. • Cerebral Embolization (Micro/Macro). • Aortic Atherosclerosis. • Air/Fat Embolism. • Haemdynamic fluctuations. • Vasculopathy (Carotis, Brain) • Systemic Inflammatory Reaction.
Neurological Outcome Only few prospective Randomized Trials showed superiority of OPCAB Vs CABG. 1. Sedrakan - Stroke 2006 41 randomized trials – 50% reduction of stoke in OPCAB 2. Glenville – Ann. Thor. Surg. 2004 Elderly P. Stroke CABG – 3% OPCAB 1% 3. Mohr – Ann. Thor. Surg. 2003 16,184 p. Stroke CABG - 3.8% OPCAB 1.9% Others 1. Alamanni – Eur. J. Cardioth. Surg. 2007 No difference stroke rate 2. Lund – Ann. Thorac. Surg. 2005 No difference in long term cognitive function or MRI evidence of brain injury On the Other Hand Puskas – Ann. Thor. Surg. 2000 In series of 10,800 p. found 3 independent variables for prediction of stroke – age, previous Tia, carotid bruit
Respiratory Outcome In a large series of patients with high respiratory risk : ventilation time significantly shorter after OPCAB Reddy. Eur. J. Cardthor. Surg. 2006 Other Trials resulted in same conclusions.
Myocardial Outcome Some large prospective randomized studies revealed less myocardial injury after OPCAB. Rastan – Eur. J Cardioth. Surg. 2005
Inflammation Mechanism of inflammation on pump Contact activation of Ischemia-Reperfusion Translocation of immune system injury to brain, kidney endotoxins through following exposure liver, heart, lung damaged mucosal of blood to foreign bowel. barriers. surfaces of pump. Activation of inflammatory cascade Post pump disease
Inflammation Not found correlation between clinical outcome and inflammation response nevertheless strong evidence of cytokines cascade during pump. -Wan – J. Thor. Card. Surg. 2004. Intense inflammatory response – Interleukin 6, 8, 10, TNFα, Vascular adhesion molecule 1, complement activation. -Luyten – Eur. J. Cardioth. Surg. 2005. Systemic inflammation caused by oxidative stress due to ischemia generated oxidative products which caused endogenous antioxidants. WHO IS GUILTY? PUMP? SURGERY ITSELF? YET NOT CLEAR
Blood Loss + Transfusions • Clear evidence in reduction of blood loss in OPCAB. Ascine – Eur. J. Cardioth. Surg. 1999 • Clear evidence in reduction of transfusions in OPCAB. Puskas – Ann. Thor. Surg. 1998
Graft Patency • Few prospective randomized studies documented reduction of graft patency rate in OPCAB. • Parolari – Ann. Thor. Surg. 2005 • Other large trials present similar patency in OPCAB Vs. CABG • Puskas – JAMA 2004 • Fukui – Ann. Thor. Surg. 2007 • Calafiore – Ann. Thor. Surg. 1999 • Jansen – J. Thor. Cardiovasc. Surg. 1998
An example of outcome between CABG Vs. OPCAB is presented in substudy of “Care Registry” CABG OPCAB No. of patients 654 597 Mean no. of grafts 3.4 +1 2.9+1.2 Op. Mortality 1.7% 1.7% Stroke 0.9% 0.7% Reop. for bleeding 2.6% 1.0% Prolonged Ventilation 10.0% 3.4% Atrial Fibrillation 23.0% 15.0% Transfusions needed 51.0% 35.0% Hospital stay 7.5 d 6.2 d Mortality 1 y 4.9% 4.6% Myocardial Infarction 1y 1.0% 0.7% Need for Re-vascularization 2.8% 4.1% Ann. Thor. Surg. 2007
Innovations in OPCAB - Possible to operate in patients with neoplastic comorbidities. (Decrease in: inflammatory response, coagulopathy disorders, immunity response and spreading of malignancy). • Possiblity to perform in SEMI awake patient, ACAB. • Surgical comfort depends on experience. - Hybrid Re-vascularization (in the future to be performed at the same time, in the same place)
Conclusion Who should benefit from OPCAB ? A Very High Risk Patient With Severe Comorbidities. Thank you.