Download
1 / 26
460 likes | 2.36k Views
Prior to 1930's, heart surgery seen as impossible, with high morbidity and mortality

E N D
1. Coronary Artery Bypass Graft Joshua Paul Aronson
March 20, 2003
5.22J Biotechnology & Engineering
Professors J. Essigmann and R. Langer
TA: Jyoti Agarwal Cover PageCover Page
2. Go over history, summarize slide, don�t readGo over history, summarize slide, don�t read
3. Chronic angina
Unstable angina
Acute myocardial infarction
Acute failure of percutaneous transluminal coronary angioplasty (PTCA)
Severe coronary artery disease Indications for surgeryIndications for surgery
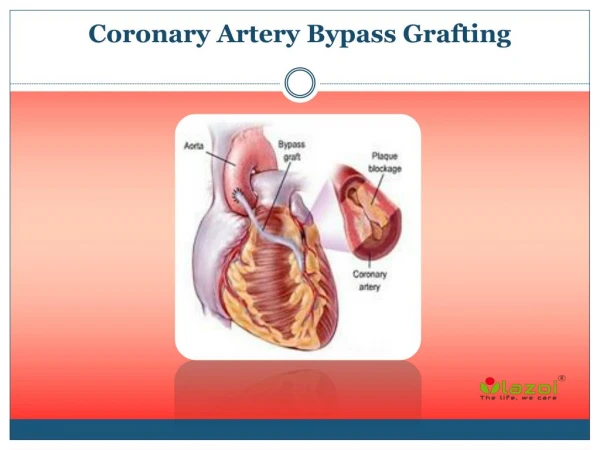
4. Most common arteries bypassed:
Right coronary artery
Left anterior descending coronary artery
Circumflex coronary artery
5. Saphenous vein used for bypassing right coronary artery and circumflex coronary artery
Internal mammary artery (IMA) used for bypassing left anterior descending coronary artery
Patency rate over 90% after 10 years
If more veins are needed, alternative sites such as upper extremity veins can be used
Patency rate as low as 47% after 4.6 years
6. Conduit removed
Median sternotomy
Sternum divided using electric saw
Cold potassium cardioplegia
Cardiopulmonary bypass
Cannulation of:
Ascending aorta
Femoral artery
Right atrium
Heparin administered to minimize clotting
7. Bypass of arteries:
Incision in target artery:
Anastamosis of graft with artery:
9. Positive:
Relief of angina in 90% of patients
80% angina free after 5 years
Survival about 95% after 1 year
Low chance of restenosis
Negative:
2-3 days in ICU, 7-10 day total hospital stay
3-6 month full recovery time
5-10% have post-op complications
High cost ($25,000-$30,000)
Long time on CPB
Depression of the patient's immune system
Postoperative bleeding from inactivation of the blood clotting system
Hypotension
10. Minimally invasive surgery does not use CPB
Smaller incision
Emerging as a replacement for conventional CABG
Starting in 1990�s, MIDCAB has gained popularity
Usually conducted for LIMA to LDA grafts
11. Additionally, MIDCAB:
Reduced need for blood transfusions, if any
Less time under anesthesia: patients are moved out of intensive care more quickly
Less pain and discomfort
Up to 40% savings over conventional CABG (under $20,000 compared to over $30,000)
12.
13. Small portion of front of 4th rib removed
LIMA clipped and dissected
MIDCAB retractor and
LIMA stabilizer
facilitates grafting
14. LAD exposed Anastamosis preformed with assistance of mechanical stabilizer
15. MIDCAB in-hospital and 1 year results (n=174)
This study conducted at Washington Hospital Center by a single surgical team
Clinical results improved with each operation performed
16. New instruments must be developed
Requires highly skilled surgeon and learning curve for surgeons limits number performed
Small incision
Beating heart
Blood in field
Can only be used with patients having blockages in one or two coronary arteries on the front of the heart
Attempts at operating on other arteries have been moderately successful, but requires even greater skill and practice
17. Uses CPB
Balloon catheter system for aortic occlusion and cardioplegic arrest
5-8 cm left anterior thoracotomy incision
No sternotomy!!!
18. LIMA harvested using specialized retractor
Aorta drawn into operating field
19. Aorta clamped, anastamosis performed
20. Benefits:
Bloodless field
Heart arrested
allows more accurate anastomoses than MIDCAB
Smaller incision than CABG
No sternotomy
Drawbacks
Uses CPB
Technically very difficult
21. Arterial Revascularization Therapy Study (ARTS) 2001
Percentage requiring second revascularization:
16.8% in stenting group
3.5% in CABG group
Event-free survival at one year:
73.8% of stent group
87.8% of CABG
Costs for the initial procedure $4,212 less for stenting
Difference reduced during follow-up because of the increased need for repeated revascularization
After one year, the net difference in favor of stenting was $2,973 per patient.
22. Stent or Surgery Study (SOS) 2001
Death rate for CABG in this study unusually low
24. CABG results in a lower restenosis rate as compared with stenting
Drug-eluting stents will narrow this difference
Due to repeat treatment, costs for stents and surgery are approximately equal after 2 years
Minimally invasive surgeries (MIDCAB and port-access) will result in fewer complications from surgery and a shorter hospital stay
This leads to lower costs for surgery, essentially removing the cost advantage of stenting
Diabetics have a substantially better response to CABG than to angioplasty and stenting
25. Currently, stenting is recommended over surgery for one-vessel disease
In the future, drug-eluting stents will probably be used
Minimally invasive surgeries could be used in place of stents in diabetic, and other high-risk patients
For more than one-vessel disease, surgery is substantially better at preventing restenosis and so will likely continue to be used in the future
Minimally invasive surgeries will expand and replace most conventional CABG procedures
26. References:
Cohen, Robbin G, et al. Minimally Invasive Cardiac Surgery. St. Louis: Quality Medical Publishing, Inc, 1999.
Gravlee, Glenn P, at al. Cardiopulmonary Bypass: Principles and Practice. Philadelphia: Lippincott Williams & Wilkins, 2000.
Holmes Jr, David R. �Debate: PCI vs CABG: a moving target, but we are gaining,� Current Controlled Trials in Cardiovascular Medicine. December 2001 Vol 2 No 6.
Harlan, Bradley J, et al. Manual of Cardiac Surgery. New York: Springer-Verlag, 1995.
Mehran, R, et al. �One-Year Clinical Outcome After Minimally Invasive Direct Coronary Artery Bypass,� Circulation. December 2000 Vol 102 Issue 23 Pages 2799-2802
Salerno, Thomas A, at al. Beating Heart Coronary Artery Surgery. Armonk: Futura Publishing Company, Inc, 2001.
Serruys, Patrick W, et al. �Comparison of coronary-artery bypass surgery and stenting for the treatment of multivessel disease,� New England Journal of Medicine. April 12, 2001 Vol 344 No 15.
Stables, RH, et al. �Coronary artery bypass surgery versus percutaneous coronary intervention with stent implantation in patients with multivessel coronary artery disease (the Stent or Surgery trial): a randomised controlled trial,� The Lancet. September 28, 2002 Vol 360 Issue 9338 Pages 965-970.
American College of Cardiology
Medscape.com
TCTMD.com
WebMD.com