Download
1 / 11
200 likes | 1.22k Views
TRIMODAL DEATH DISTRIBUTION. 50% 40% 30% 20% 10% 0%. HOURS 0 1 2 3 4 WEEKS 1 2 3 4. TRIMODAL BIMODAL? THE SECOND GROUP IS DECREASING DUE TO PROPER TREATMENT. DEFINITION OF POLYTRAUMA

E N D
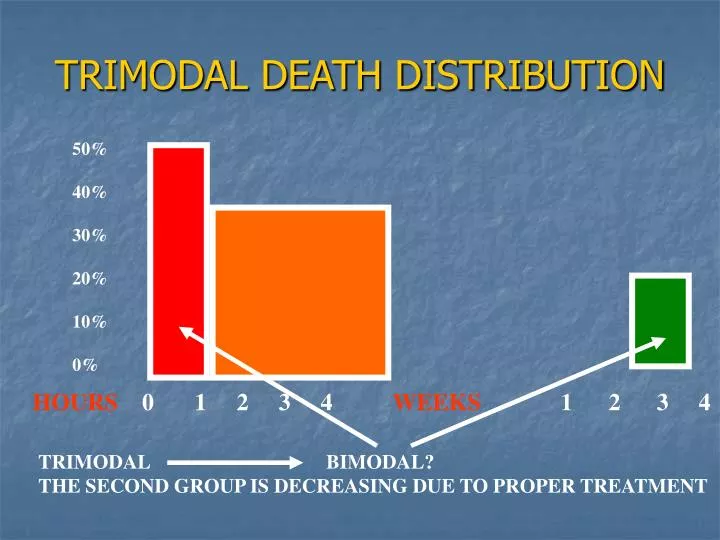
TRIMODAL DEATH DISTRIBUTION 50% 40% 30% 20% 10% 0% HOURS 0 1 2 3 4 WEEKS 1 2 3 4 TRIMODAL BIMODAL? THE SECOND GROUP IS DECREASING DUE TO PROPER TREATMENT
DEFINITION OF POLYTRAUMA • A. INJURY TO ONE OR MORE BODY REGIONS OR ORGANS OF WHICH ONE, OR THEIR COMBINATIONS IS LIFE THREATENING • INJURY TO MORE BODY REGIONS FOLLOWING WHICH, DURING TREATMENT, WE HAVE TO MAKE COMPROMISES • INJURY TO HOLLOW ORGANS + INJURY TO EXTREMITIES • INJURY DEFINED BY SCORING SYSTEM
INJURY SEVERITY SCORE (ISS) • SIX REGIONS • THE THREE MOST SEVERE • THE SQUARE OF EACH VALUE • THE SUM OF THE RESULTS • HEAD AND NECK • FACE • CHEST • ABDOMEN • EXTREMITIES (PELVIS) • SKIN
DEFINITION OF POLYTRAUMA • A. INJURY TO ONE OR MORE BODY REGIONS OR ORGANS OF WHICH ONE, OR THEIR COMBINATIONS IS LIFE THREATENING • INJURY TO MORE BODY REGIONS FOLLOWING WHICH, DURING TREATMENT, WE HAVE TO MAKE COMPROMISES • INJURY TO HOLLOW ORGANS + INJURY TO EXTREMITIES • INJURY DEFINED BY SCORING SYSTEM
ATLS CONCEPTIONADVANCED TRAUMA LIFE SUPPORTABCDE APPROACHFIRST THE LIFE THREATENING INJURYTHE IMMEDIATE EXACT DIAGNOSIS IS NOT IMPORTANTTHE TIME FACTOR IS THE MOST IMPORTANTDO NOT DO MORE HARM
THE CAUSE OF SHOCK BLEEDING NON BLEEDING BLEEDING TENSION PTX (FAST)CARDIAC TAMP. FOCUSED CARDIOGENIC ASSESSMENT NEUROGENIC SONOGRAPHY in SEPTIC TRAUMA CHEST, PELVIS X-RAY
PATIENT RESPONSE „RAPID RESPONDER” CRISTALLOIDS „TRANSIENT RESPONDER” CRISTALLOIDS, TRANSFUSION PATIENT RESPONSE? „NON-RESPONDER” CRISTALLOID, IMMEDIATE TRANSFUS. SURGERY
SECONDARY SURVEY AMPLE A ALLERGIES M MEDICATIONS P PAST ILLNESSES L LAST MEAL E EVENTS/ENVIRONMENT
THERAPEUTIC WINDOWS • FIRST 24 (48) HOURS • 5-7 DAYS FOLLOWING INJURY • 2-3 WEEKS • ABDIMINAL THORACIC, BRAIN INJURIES • EXTREMITIES • VESSEL, NERVE INJURIES • INTRAMEDULLARY STABILISATION • EXTERNAL FIXATEUR
MOF AND SIRS • MULTIPLE ORGAN FAILURE • SYSTEMIC INFLAMMATORY RESPONSE SYNDROME • MOF • HYPOXIA, HYPOPERFUSION, („FIRST HIT”) • BACTEREMIA TOXINS – BOWEL HYPOPERFUSION („SECOND HIT”) • FRACTURE OF LONG TUBULAR BONES • MEDIATORS • SIRS TWO OR MORE OF THESE FACTORS • FEVRE HIGHER THAN > 38 OR < 36 • TACHYPNOE > 24/MIN • TACHYCARDIA > 90/ MIN • LEUCOCYTOSIS >12 000/ MM3 • LEUCUPENIA > 4000 OR JUVENILE CELLS MORE THAN 10% SHOCK
TRIAGE • DEGREE OF LIFE THREAT POSED BY THE • INJURY • INJURY SEVERITY • SALVAGEABILITY • RESOURCES AVAILABLE • TIME, DISTANCE, ENVIRONMENT