Download
1 / 50
520 likes | 625 Views
Understand the embryology, anatomy, and development of the prostate gland. Explore how the gland forms, its role in enzyme synthesis, and normal anatomy. Learn about zonal anatomy, lobar concept, and McNeal's zone theory.

E N D
ZONAL ANATOMY OF PROSTATE Dr Ankush Jajodia
Embryology and development of the prostate gland • During the third month of gestation the prostate gland develops from epithelial invaginations from the posterior urogenital sinus under the influence of the underlying mesenchyme . • Formation of the prostate : by proliferation of the epithelium of the posterior urethra around the orifices of the Wolffian canal to surround the urethral circumference. The prostatic glands formed anterior to the urethra regress and are replaced by fibromuscular stroma. The secretory function of the glands starts about the 13th week of gestation.
Role of enzyme • The normal formation of the prostate gland requires the presence of 5α-dihydrotestosterone, which is synthesized from fetal testosterone by the action of 5α-reductase . • This enzyme is localized in the urogenital sinus and external genitalia of humans . Consequently, deficiencies of 5α-reductase will cause a rudimentary or undetectable prostate in addition to severe abnormalities of the external genitalia, although the epididymides, vasadeferentia, and seminal vesicles remain normal
During the prepubertal period, the constitution of the human prostate remains more or less identical but begins to undergo morphologic changes into the adult phenotype with the beginning of puberty. The gland enlarges continuously in size to reach the adult weight of approximately 20 g by 25–30 years of age
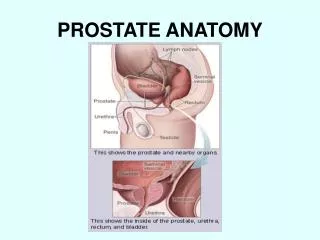
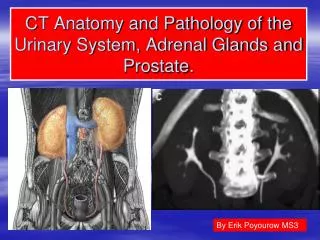
Normal anatomy of the prostate • The base of the prostate is at the bladder neck and the apex at the urogenital diaphragm . • The Denonvilliers’ fascia, a thin, filmy layer of connective tissue, separates the prostate and seminal vesicles from the rectum posteriorly. • Skeletal muscle fibers from the urogenital diaphragm extend into the prostate at the apex and up to the midprostate anteriorly.
The histologic architecture of the prostate is that of a branched duct gland. • Two cell layers, a luminal secretory columnar cell layer and an underlying basal cell layer, line each gland or duct. • The lumens of otherwise normal prostatic glands and ducts frequently contain multilaminatedeosinophilic concretions, termed corpora amylacea, that become more common in older men. • Calculi are larger than those corpora with a predilection for the ducts that traverse the length of the surgical capsule, separating the transition and peripheral zones.
Lobar concept of intraprostatic anatomy • In 1912, Lowsley demonstrated the first detailed description of the anatomy of the prostate. • This traditional concept which is no longer used, divided the prostate into lobes: an anterior,posterior, middle and two lateral lobes. This method has been used to identify the prostate and prostatic disease for about 60 years.
The anterior lobe was situated from the anterior margin of the gland to the level of the prostatic urethra. • The middle lobe was a small area between the proximal prostatic urethra and the ejaculatory ducts. This lobe extnds form the base of the prostate to the level of verumontanum. • The posterior lobe was situated posterior to the ejaculatory ducts and extends to the posterior margin of the gland. • The two lateral lobes extend from the lateral margin of the gland bilaterally toward the middle part of the gland. None of these lobes has clearly defined medial margin
McNeal established the current and most widely accepted concept of various zones rather than lobes of the prostate • Peripheral zone • Transition zone • Central zone • Anterior fibromuscular zone
These zones have differing embryologic origins and susceptibilities to disease . • In the normal young man’s gland, however, sonography can rarely identify these zones separately unless a pathologic condition is present . • On sonography, it is more useful to consider the prostate as having a peripheral or outer gland (peripheral zone + central zone) and inner gland (transition zone + anterior fibromuscular stroma + internal urethral sphincter).
The peripheral zone • largest of the glandular zones, contains approximately 70% of the prostatic glandular tissue in a young man before the onset of benignprostatic hyperplasia (BPH) and is the site for about 70% of prostate cancers. • Its ducts open into prostatic urethra distal to verumontanum. • It surrounds the distal urethral segment and is separated from the transition zone and central zone by the surgical capsule which is usually seen as a hypoechoic line but may be rendered hyperechoic by the frequent accumulation of corpora amylacea or calcifications along this line.
Traditionally, urologists at the time of suprapubic resection (or transurethral resection of prostate) believed that they dissected to this line; thus the designation “surgical” capsule. • The peripheral zone occupies the posterior, lateral, and apical regions of the prostate, extending somewhat anteriorly, resembling an eggcup holding the “egg” of the central gland. • In this zone, carcinoma, chronic prostatitis, and postinflammatory atrophy are relatively more common than in the other zones.
The central zone • 25% of the glandular tissue. • It is wedge shaped at the prostate base between the peripheral and transition zones. • The ducts of the vas deferens and seminal vesicles enter the base of the prostate at the central zone, where they are renamed the ejaculatory ducts and pass through it en route to the seminal colliculus (crest) or verumontanum .
The central zone is thought to be relatively resistant to disease processes and is the site of origin of only about 5% of prostate cancer. • At the base of the prostate is the thick, muscular, continence-providing internal urethral sphincter. • Its substantial muscular content can make it appear hypoechoic. It contains periurethral glands that often contain calcifications.
The transition zone • in a young man contains approximately 5% of the prostatic glandular tissue. • It is seen as two small glandular areas positioned like saddlebags adjacent to the proximal urethral sphincter. • Its ducts open in postrolateral part of urethra • The transition zone is the site of origin of most BPH and about 20% of prostate cancer.
Fibro-muscular zone • The anterior fibromuscularstroma (AFMS) forms the convexity of the anterior external surface. The apical half of this area is rich in striated muscle, which blends into the gland and the muscle of the pelvic diaphragm . • Toward the base, smooth muscle cells become predominant, blending into the fibers of the bladder neck . • The distal portion of the AFMS is important in voluntary sphincter functions, whereas the proximal portion plays a central role in involuntary sphincter functions.
Axial Ultrasound Anatomy • The inner transition zone is separated from the peripheral zone by the usually hypoechoic surgical capsule . • This line becomes obvious as BPH enlarges the transition zone. Often corpora amylacea seen as echogenic foci, develop along the surgical capsule. • Frequently, in young men, no clear separating line is seen between the zones . • The peripheral zone has a uniform, homogeneous texture and is slightly more echogenic than the transition zone. • The peripheral zone echogenicity is taken as the standard for echogenicity in the prostate and is defined to be isoechoic..
Echogenicity in other areas of the gland is compared tothat of the peripheral zone. Laterally, the peripheral zonecurves anteriorly to enclose the transition zone; thisupward curved part was named the “anterior horns” because it resembled the hornsof a steer. • The margin of the prostate forms a clear interfacewith the periprostatic fat except posterolaterally,where vessels enter the prostate and make the marginindistinct, an appearance that can mimic tumor extensionthrough the capsule. • Prominent veins of Batson’s venousplexus are visible in the periprostatic fat, sometimes containingcalcified shadowing phleboliths.
Sagittal Ultrasound Anatomy • On midsagittal view the muscular internal urethral sphincter can be seen extending from the bladder to verumontanum. • When corpora amylacea fill the periurethral glands, they may form a linear hyperechoic configuration . • The anterior fibromuscular zone forms an inconspicuous area anterior to the internal sphincter. • At the verumontanum, the distal urethra angles slightly anteriorly and ultimately exits the apex of the prostate just before it enters the urogenital diaphragm, which is the external urethral sphincter. • In the true midline the apex can be difficult to identify because it blends with the urethra. Often, a subtle bulge just at the junction helps to identify it. When measuring the head-to-foot length of the prostate, the scan plane can be shifted minimally to one side of this apical urethra to identify the apex more clearly.
In the midplane the ejaculatory ducts are visible as hypoechoic tracts extending from the vas deferens at the base to the centrally located verumontanum. • Parasagittally in men with hyperplasia the anterior hyperplastic transition zone can be seen separated from the posteriorly situated peripheral zone by the surgical capsule. • The vas deferens and seminal vesicles are visible above the base. • Still more laterally, the transition zone ends, leaving only the part of the peripheral zone that curves anteriorly at the sides of the glands (anterior horns). • With BPH, the transition zone enlarges anterolaterally and compresses the peripheral zone into a thin, posterior rim.
Correlation of the lobar and zonal concepts of anatomy of the prostate • A comparison of Lowsley lobar and McNeal zonal concepts of anatomy is possible and important to compare the clinical findings. • Clinicians may still refer to lobar anatomy while radiologists use zonal anatomy. • So, the anterior lobe correlates with the anterior fibromuscular stroma. The medial lobe and the CZ are similar. The sum of the posterior and two lateral lobes correlated to a large extent with the PZ.
Prostatic capsule • composed of fibrous tissue surrounding the gland. • Although the term “capsule” is embedded in the current literature there is no consensus about the presence of a true capsule . This capsule is best appreciated posteriorly and posterolaterally as a layer more fibrous than muscular, between the prostatic stroma and extraprostatic fat.
Seminal vesicles • located superior to the base of the prostate. • They undergo confluence with the vas deferens on each side to form the ejaculatory ducts. The ejaculatory duct complex consists of the two ejaculatory ducts along with a second loose stroma rich in vascular spaces. • The utricle (when present) is located between the ejaculatory ducts. The remnants of the utricle occasionally form cystic structures in the midline posteriorly. • The seminal vesicles are resistant to nearly all of the disease processes that affect the prostate. Seminal vesicle involvement (SVI) by prostate cancer (PCa) is one of the most important predictors for PCa progression
TRANSABDOMINAL TECHNIQUE • The patient lies supine. • The patient should have a half full bladder . • The probe is angled approximately 30 degrees caudal using the bladder as a window. • Slight compression to ensure the inferior portion of the prostate is not obscured by the shadow artifact from the base of the bladder.
TRUS TECHNIQUE • It is ideal to have a small amount of urine in the bladder. • Ask the patient to try and relax and "bear down" to open the sphincter as the transducer is inserted slowly. • Ensure the transducer has a latex free dedicated probe cover with plenty of gel. The highest frequency sector probe 7-12MHz should be used. • The scanning begins in the axial plane. The seminal vesicles are examined initially. As the probe is angled caudally the base of the prostate is seen. Once the prostate is examined in its entirety in this plane the probe is turned 90degrees in a sagittal plane. The probe is angled from one side across to the other. • A volume is taken by measuring height x length in the sagittal plane and x width in the axial plane and multiply by 0.52. • Look for changes in the contours and echogenicity in each zone.
TRUS was initially considered a primary screening test for prostate cancer. • This role has now been replaced by prostate-specific antigen (PSA) and digital rectal examination (DRE). • Also, most prostate cancers occur posteriorly, where transvesical scanning cannot see them.
Purpose of The Transrectal Ultrasound: (“TRUS”) • Assist In Obtaining Prostate Biopsies (“Bx”) • Targeting Of Suspicious Areas • Guidance For Systematic Biopsies
TRUS – Additional Information • Prostate Size Estimate • PSA Density • The Relationship Of The PSA To Prostate Size • Identify Benign Causes Of Abnormal Digital Rectal Exam • Calcium Deposits • Cysts • Shape Irregularities
PROSTATE MRI ANATOMY • On T1‐weighted MR images the normal prostate gland demonstrates homogeneous intermediate to low signal intensity. • However T1‐weighted MR imaging has insufficient soft‐tissue contrast resolution for visualizing the intraprostatic anatomy or abnormality. • The zonal anatomy of the prostate gland is best depicted on high‐resolution T2‐weighted images. • On T2‐weighted images, the normal peripheral zone demonstrates a high signal intensity. The signal intensities in the central and transition zones are lower than those in the peripheral zone. • The anterior fibromuscular stroma has low signal intensity.
MR‐Spectroscopy of the Prostate • prostate cancer is characterized by elevated levels of choline (a normal cell membrane constituent, which is elevated in many tumors) or reduced levels of citrate (a constituent of normal prostatic tissue) or both. • The ratio of choline and creatine to citrate in normally healthy prostatic tissue has been established as 0.22 +/‐ 0.13.
Evaluation of MR Images in Prostate Carcinoma • Carcinoma usually from PZ – appear as hypointense lesion. • Extracapsular extension : irregular bulging of the prostatic outline, breach of the capsule with extracapsular spread, asymmetry of the neurovascular bundles, and loss of the rectoprostatic angle. • Invasion of seminal vesicles ‐ Contiguous areas of low signal intensity extending into the seminal vesicles from the base of the prostate (Note – this also may be seen postradiotherapy & post‐biopsy) • Invasion of bladder/rectum • Lymph nodes – lymph nodes >1 cm considered involved