Download
1 / 7
70 likes | 264 Views
Validation of a depression screening tool for use with Aboriginal and Torres Strait Islander Australians Presented by A/Prof Maree Hackett On behalf of : Prof Alan Cass, Prof Nick Glozier, Prof Timothy Skinner, Dr Armando Teixeira-Pinto, Dr Deb Askew, Prof Alex Brown & Mr Graham Gee.

E N D
Validation of a depression screening tool for use with Aboriginal and Torres Strait Islander Australians Presented by A/Prof Maree Hackett On behalf of: Prof Alan Cass, Prof Nick Glozier, Prof Timothy Skinner, Dr Armando Teixeira-Pinto, Dr Deb Askew, Prof Alex Brown & Mr Graham Gee
I would like to show my respect and acknowledge the Traditional Custodians of the Land, of Elders past and present, on which this meeting takes place
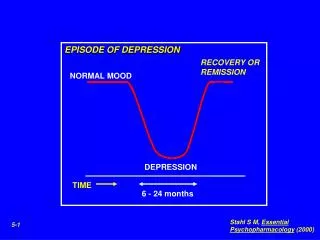
Depression One of the leading causes of disability (YLD) Only recognised in up to ½ of cases (often present with physical symptoms) People living with depression have risk of premature death x2 population Doubles the risk of a first and subsequent cardiovascular event Research on potential mechanisms (inflammation, coagulation, emotional triggers of plaque rupture, lack of adherence to secondary prevention, inability to make lifestyle/behavioural changes…) No research with Aboriginal and Torres Strait Islander people No validated, free, measure of depression for use with Aboriginal and Torres Strait Islander people Aboriginal and Torres Strait Islander people 3-4x more likely to die from CV conditions than non-Indigenous
Prof. Alex Brown’s PhD work • Translation and adaption of PHQ-9 depression screener • within and across 5 primary Aboriginal languages • in Central Australia, with Aboriginal men • iterative process over 12 months • Some concepts unfamiliar: hopelessness • Others consistent: depression • Questions covered opposing concepts were split • Time frame (previous 2 weeks) and severity grading was understood Original PHQ-9 Brown et al. BMC Psychiatry 2013, 13:271 http://www.biomedcentral.com/1471-244X/13/271
Original PHQ-9 Adapted PHQ-9 wording
Validation study details • Setting: Aboriginal Medical Services in Australia (aiming for 10 high recruiting centres) • Design: Observational, cross sectional, validation study • Participants: Identify as Aboriginal or Torres Strait Islander, ≥ 18 years, 1 attendance at AMS in previous year, with or without chronic disease, can give informed consent • Baseline assessment: Demographics, history of depression, chronic disease history • Measure for validation: aPHQ-9 (paper or iPad) + 7 additional questions • Gold standard: Composite International Diagnostic Interview for depression (CIDI) • Primary Outcome: Criterion validity of aPHQ-9: sensitivity, specificity, positive and negative predictive values • Secondary Outcomes: Determine contribution of 7 additional questions to the identification of depression • Statistical analysis: Assuming major depression prevalence of 10% (CIDI), sensitivity of 0.85, 500 people, ~precision of 0.1 using usual ≥ 10 cut point score on the aPHQ-9 • Other cut points will be explored using ROC curves • Sensitivity and specificity for subgroups (with and without chronic disease, history of depression) • ROC curves compared with the addition of each of the 7 questions using a stepwise strategy