Download
1 / 46
470 likes | 510 Views
DIURETICS Part 1. Prof. Hanan Hagar Pharmacology Department. Diuretics Are drugs that increase renal excretion of sodium and water resulting in increase in urine volume. Most diuretics act by interfere with the normal sodium handling by the kidney. Sites of action for diuretics

E N D
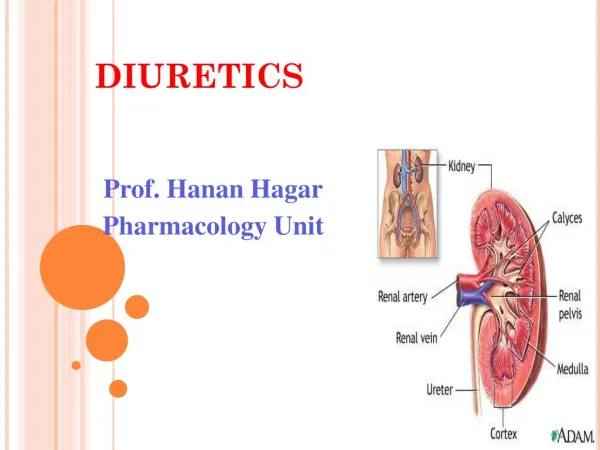
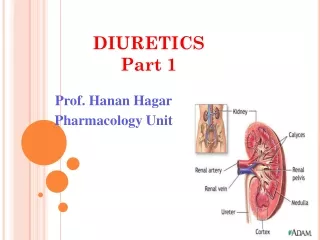
DIURETICSPart 1 Prof. Hanan Hagar Pharmacology Department
Diuretics • Are drugs that increase renal excretion of sodium and water resulting in increase in urine volume. • Most diuretics act by interfere with the normal sodium handling by the kidney.
Sites of action for diuretics • Target molecules for diuretics are specific membrane transport proteins in renal tubular epithelial cells (transporters).
Classification of diuretics • Carbonic Anhydrase Inhibitors • Loop Diuretics • Thiazides • Potassium-Sparing Diuretics • Osmotic Diuretics
kidney • Nephron is the unit of the kidney • It is classified structurally and functionally into different zones • Glomerulus • Proximal convoluted tubule • Descending loop of Henle • Ascending loop of Henle • Distal convoluted tubule • Collecting duct
FUNCTION OF THE KIDNEY • Kidney is responsible for regulation of fluids and electrolytes. • Kidney do its function through three processes • Glomerular filtration • Passive tubular re-absorption • Active tubular secretion
Glomerular filtration: • 16-20 % of blood entering the kidney is filtered • Filtrate contains water, glucose, amino acids, sodium bicarbonates, organic solutes and electrolytes (sodium, potassium, chloride).
Proximal convoluted tubules: • Responsible for re-absorption of • all glucose, amino acids • organic solutes • electrolytes as • sodium chloride (NaCl)(66% of Na) • sodium bicarbonate (NaHCO3,85%) • Potassium (K+, 66 %)
Proximal convoluted tubule (PCT): • HCO3- is reabsorbed by action of enzyme carbonic anhydrase (luminal membrane of proximal tubular cells). • Water (passively following salts to maintain osmolarity in tubular fluids (60%). • PCT is the site of organic acids or bases secretory systems
carbonic anhydrase Lumen Blood Luminal membrane Basolateral membrane
organic acids or bases secretory systems • Organic base secretory system responsible for secretion of bases into luminal fluid e.g. choline and creatinine • Organic acid secretory system responsible for secretion of acids into luminal tubular fluid e.g. uric acid, NSAIDs, antibiotics and diuretics.
Descending loop of Henle In thin descending loop of Henle : water is re-absorbed by osmotic forces in hypertonic medullary interstitium (counter current mechanism)
Ascending loop of Henle • Is impermeable to water • In thick ascending loop of Henle (TAL)is responsible for active re-absorption of Na, K and Cl (25-30% Na) via transport system in luminal membrane called Na+/ K+ / 2Cl- co-transporter • TAL is called the diluting segment • Ca and Mg enter the interstitial fluid via paracellular pathway
Distal convoluted tubule (DCT) • Is impermeable to water • Responsible for active re-absorption of NaCl (10%) via transport system Na/Cl transporter in luminal membrane • Ca2+ actively reabsorbed via apical Ca channel and Na+/Ca2+ exchanger in basolateral membrane
Collecting tubule • Principal cells are responsible for re-absorption of Na (in exchange for K via Na/K-ATPase) and water • Aldosterone receptors located in the principle cells influence Na re-absorption and K secretion • Intercalated cells affect H secretion • Water re-absorption (anti-diuretic hormone, ADH).
Carbonic Anhydrase Inhibitors Acetazolamide – dorzolamide Mechanism of action: Inhibits carbonic anhydrase (CA) enzyme in PCT thus interferes with NaHCO3 re-absorption and causes diuresis. CA is required for reversible reaction, in which CO2 +H2O ↔ H2CO3
Blood Lumen Basolateral membrane Luminal membrane
Pharmacological actions: • ↑ urinary excretion of bicarbonate, sodium, potassium “alkaline diuresis” • Metabolic acidosis. • ↑ urinary phosphate excretion. • Weak diuretics. • Decreases after several days (self-limiting as the blood bicarbonate falls).
Pharmacokinetics: • given orally once a day. • Onset of action is rapid (30 min). • Duration of action (12 h). • Excreted by active secretion in proximal convoluted tubules forming alkaline urine
Therapeutic uses: • Open angle glaucoma (↓ IOP by reducing aqueous humor formation via blocking carbonic anhydrase in ciliary body of eye). • As prophylactic therapy, in acute mountain sickness (to decrease CSF and pH of brain).
Therapeutic uses: • Urinary alkalinization to enhance renal excretion of acidic substances (uric acid and cysteine in cystinuria). • Epilepsy (decrease cerebrospinal fluid, CSF). • Hyperphosphatemia • Metabolic alkalosis
Adverse effects: • Hypokalemia (potassium loss). • Metabolic acidosis. • Renal stone formation (calcium phosphate stones). • Hypersensitivity reactions
Dorzolamide • Is a carbonic anhydrase inhibitor • Used topically for treatment of increased intraocular pressure in open-angle glaucoma. • no diuretic or systemic side effects (Why?).
LOOP DIURETICSHigh Ceiling diuretics • The most efficacious diuretics Efficacy: High 25-30% natriuresis Drugs as • Furosemide - torsemide • Bumetanide - Ethcrynic acid
LOOP DIURETICS Mechanism: • inhibit Na+ / K+ / 2 Cl- co-transporter in the luminal membrane of the thick ascending loop of Henle (TAL). • inhibit Ca++ and Mg ++ re-absorption.
Pharmacokinetics • Given orally or I. V. • Has fast onset of action (suitable for emergency) • Have short duration of action. • Excreted by active tubular secretion of weak acids into urine (compete with uric acid for renal secretory system).
Pharmacological effects: • ↑ urinary excretion of Na+ , K,+ Ca++ and Mg ++ • ↑ urine volume • ↑ renal blood flow.
Uses: are drug of choice for emergency situations as: • Acute pulmonary edema • Edema associated with heart failure, nephrotic syndrome • Acute hyperkalaemia. • Acute hypercalcemia
Adverse effects : • Hypokalemia (dietary K supplementation or K-sparing diuretics). • Metabolic alkalosis. • Acute Hypovolemia, postural hypotension
Adverse effects : • Hyponatraemia. • Hypomagnesaemia • Hyperuricemia (increase gouty attack). • Ototoxicity (risk increased if combined with aminoglycosides) • Allergic reactions