Download
1 / 35
360 likes | 420 Views
Epstein Barr Virus [EBV] - Named after Epstein and Barr. Observed the virus under EM from cultures of lymphoblasts derived from Burkitt’s lymphoma. It is implicated in Burkitt’s lymphoma, B cell lymphomas, nasopharyngeal carcinoma.

E N D
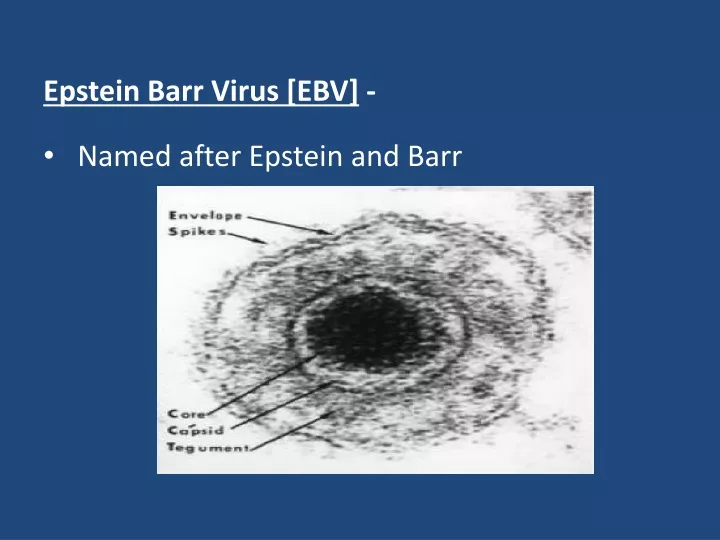
Epstein Barr Virus [EBV] - • Named after Epstein and Barr
Observed the virus under EM from cultures of lymphoblasts derived from Burkitt’s lymphoma. • It is implicated in Burkitt’s lymphoma, B cell lymphomas, nasopharyngeal carcinoma.
Associated with nonmalignant lesion on the tongue called hairy leukoplakia – in AIDS patients. • Causes infectious mononucleosis kissing disease or glandular fever: common in teenagers
Important properties- • EBV is structurally and morphologically identical to other herpes virus but is antigenically different. • Has a LMP antigen - used in diagnostic tests. • The early antigens [EA] produced prior to DNA synthesis. • EB DNA – nuclear antigen helps in diagnosis.
EBV replicates in the nasopharyngeal epithelial cells, salivary glands [Parotids] • Lyses the cells and are released in the saliva • When B cell is infiltrated it is also a target and gets infected. • Latencyin B cells: – forms a hybrid with B cell genome.
Multiple copies of EBV DNA is found in cytoplasm of infected B cell. • The latently infected cells can also be activated – B cell then can secrete IgM. • It has glycoprotein envelope gp350/220 which mediates attachment to CD21 receptor on susceptible cell – C3d receptor of the cell. • Humans are natural host.
Pathogenesis and Immunity- • Infection in oropharynx [epithelium or lymphoid tissue?] – Spread to blood – Infect B lymphocyte – Cytotoxic T cells attack infected B lymphocytes. • These T cells are atypical lymphocytes[Downey cells]seen in blood smear. • EBV can remain latent in B lymphocytes, few copies of EBV DNA integrated to cell genome. • Many copies of circular EBV DNA also found in the cytoplasm.
Heterophile means antibody that are detected by tests using antigen different from the antigens that induced them. (Paul Bunnel test)
These antibody do not react with any component of EB virus. • Likely explanation is EBV infection modifies a cell membrane constituent so that it be comes antigenic and induces heterophile antibodies. • Usually heterophile antibody disappears within 6 months after recovery. • These are not specific for EBV as they can also be found in Hep B and serum sickness.
Most shedding of virus occur in the oral cavity. So contact with saliva – kissing, contaminated eating utensils transmit. • Common world wide • During childhood most infection are asymptomatic • In adolescents it causes infectious mononucleosis or glandular fever. • In immunocompromised it has oncogenic potential and causes Burkitts lymphoma, naso pharyngeal carcinoma [China], thymic carcinoma [USA].
Infectious mononucleosis – 15-25 age group • Incubation period 4-7 weeks. • Sore throat exudative tonsillitis, generalised lymphadenopathy, fever, malaise headache, sweating, fatigue, G-I discomfort. • Sometimes liver, spleen enlarged • A maculopapular rash follows treatment with ampicillin • This is due to immune complexes with antibody to Ampicillin.
So contraindicated. • Lasts for 2-3 weeks • Complications – GuillainBarre syndrome, Bells Palsy, meningo encephalitis, transverse myelitis, hemolytic anemia, thrombocytopenia, carditis, nephritis, pneumonia and splenic rupture.
Infection in immunocompromised- • a. X-linked lympho proliferative syndrome in male. (X-linked recessive immune deficiency) • There is deficiency in synthesizing interferons. • 50% boys die within a month due to sepsis, haemorrhages and rest of them develop or die from B cell lymphoproliferation usually associated with hypogammaglobulinemia and later lymphoma.
b. EBV may cause progressive lymphoproliferative disease in transplant recipients, immunodeficient children and in AIDS patients.
EBV associated malignancies: • 1. Burkitt’s lymphoma – malignant B cell lymphoma seen in equatorial Africa, New Guinea where malaria is hyperendemic. • EBV is usually acquired early in life. • Malaria is the co-factor which potentiates the oncogenic potential of virus from B cell. • EBV genome DNA has been found as an episome in the African Burkitt’s, lymphoma cells. • The cells themselves do not produce virions. • But if grown, in vitro virions are produced.
2. Nasopharyngeal carinoma – Racial and geographical. • Seen in Chinese, Eskimos, Green landers. • Virions have been isolated form the malignant epithelial cells. 3. B cell lymphoma – Immunodeficient patients eg. HIV patients, transplant recepients may develop these lymphomas. 4. Oral hairy leukoplakia – In HIV patients, capsid of EBV seen in affected tissues. 5. Thymic carcinoma – seen in USA.
Lab diagnosis- • Hematological approach – absolute lymphocytosis10,000 – 20,000 cells/ cumm • Mainly lymphocytes and monocytes 20-30% or more ‘atypical ‘ • These are large pleomorphic blasts with deeply basophillic vacuolated cytoplasm and globulated nuclei. • These are present in blood for 2 weeks or months [these are cyto - Tcell]
2. Immunological approach – Infectious mononucleosis is accompanied by heterophileaggluttinins. • These are IgM elicited by EBV infection. • These appear during acute phase in about 90% of patient sera. • Peak levels in 2 weeks after onset. • Titer decrease rapidly by 4th week and not persists after 3 months.
Agglutination of sheep or horse red cells by patients serum adsorbed with guinea pig kidney cell to remove Forssman antibody is basis of test. • Tube agglutination test – Paul Bunnel test. • Not useful to detect prior infection. • Monospot test – Commercial more sensitive, more specific, cheaper than tube agglutination test.
3. EBV specific antibody detection – IgM to EBV capsid antigen by ELISA, Indirect IF. • Detects upto 4 weeks of illness. • This IgM decrease by 3 months. • Useful for diagnosis of difficult cases. • IgG VCA antibody response – detects prior infection • Certains instances - Antibody to EA and EBDNA useful.
4. Virus isolation – Saliva, throat washings can be inoculated into umbilical cord lymphocytes. • This is time consuming and expertise needed. • This is called co-cultivation and involves - immortalitation of EBV genome into cells and leads to lympoblastoid cells. • Its presence can also be detected by fluorescent antibody staining of unclear antigen. • Others –PCR DNA hybridisation. 5. Biopsy of tumours – DNA of virus stained by specific tagged antibody.
Treatment:- • No EB vaccine. • Acyclovir reduces EBV shedding during administration. • It does not prevent immortalisation of EBV- B cells. • No use in lymphomas or IM • Adoptive transfer of EBV reactive T cell is promising treatment • For EBV associated lympho proliferative disease
Malaria eradication associated with decreased incidence of Burkitt’s lymphoma. • Mass screening in China for IgA antibody to EBVAg was useful in early diagnosis of nasopharyngeal carcinoma. • 20% of Chinese with elevated IgA were biopsied and found to have carcinoma.
Other Herpes viruses • Human HSV-6 • Infects dividing CD4 + T lymphocytes. • Causes sixth disease in children (roseola infantum)
HHV-7: • Infects T cells • HHV-8: • Kaposis sarcoma ( body cavity lymphomas)
Lab diagnosis: • Peripheral blood mononuclear cells – used • Isolated from the co-cultivation with cord blood lymphs • Viral Ag then detected by IF using monoclonal Ab. • PCR – to amplify viral genome. • ELISA – detect virus Ag & Ab • Virology and clinical features similar to CMV.
HHV – 7 - Discovered is 1990. • Roseolainfantum, • Also infects T lymph using same CD4 receptor. • HSV – 8 – 1994 – Lymphotrophic rather than neurotrophic. • Kaposi sarcoma associated in HIV infected. • These people have Ab. • DNA a aplification by PCR is method of choice • 2% of general population have Ab. • Herpes B – simian virus – Occasionaly infect man • Usually fatal encephalitis.
Occupational risk in zoo keepers and cell culture technicians. • Latent infection in monkeys. • Herpes B and HSV-1 cross react antigenically but HSV-1 does not protect from encephalitis from Herpes B. • HSV-1 Ab confuse serologically – increase in Ab titer difficult to interpret.
Recovery of virus is specific diagnosis. • Acyclovir beneficial. • Prevention – monkey bite, mask, clothing. • Immunoglubulin containing Ab to Herpes B to be given after monkey bite • Macrophages are also infected so act as reservoir. • Isolation from saliva.