Download
1 / 31
310 likes | 539 Views
Bones of the Foot (1). 26 bones Phalanges = 14 Numbered 1-5 (big toe = Hallux = #1) distal Interphalangeal joint (DIP) proximal interphalangeal joint (PIP) Metatarsal phalangeal joint (MP) Metatarsals (numbered 1-5). Bone of the foot (2). Tarsals- Fig 12-2 Calcaneous (heel bone)

E N D
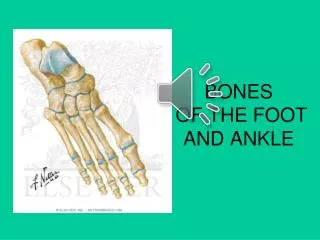
Bones of the Foot (1) • 26 bones • Phalanges = 14 • Numbered 1-5 (big toe = Hallux = #1) • distal Interphalangeal joint (DIP) • proximal interphalangeal joint (PIP) • Metatarsal phalangeal joint (MP) • Metatarsals (numbered 1-5)
Bone of the foot (2) • Tarsals- Fig 12-2 • Calcaneous (heel bone) • Talus (main weight bearing) • Navicular- medial • 3 cuneiforms • Cuboid-lateral
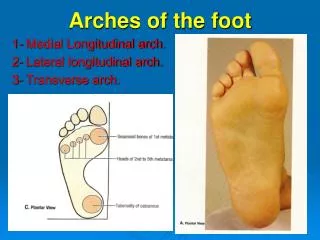
The arches Fig 12-10 • Function to support and distribute body weight • Three arches: Fig 12-10 • Medial longitudinal (higher) • supported by calcaneal-navicular ligament (spring) • Lateral longitudinal • Transverse • Plantar Fascia • Supports longitudinal arch
The Ankle Fig 12-1/12-3 • Ankle joint = talocrural joint • Three bones • Tibia (medial malleolus)-major weight bearing • Fibula (lateral malleolus) • Talus • Hinge joint • Dorsi-Flexion • Plantar Flexion
Subtalar Joint • The joint between the talus and the calcaneous • Shifts during weight bearing (WB) • Supination/inversion • Pronation/eversion
Tibiofibular Joint -Fig 12-3 • Composed of Tibia and Fibula • Ligaments/Membrane • Anterior Tibofibular Lig • Posterior Tibofibular Lig • Interosseious membrane- connects the tibia and fibula; runs the entire diaphysis of both bones
Ankle ligaments (1) – Fig 12-3 • Medial • Deltoid ligament -4 parts • Triangular shape (very strong) • Lateral • Anterior talofibular (ATF) • Calcaneofibular (CF) • Posterior talofibular (PTF) • Ankle and foot are composed of numerous ligaments; where ever two bones meet
Muscles of the Lower Leg • Thick sheaths of fascia divide muscles into 4 compartments • Anterior Compartment • Dorsiflexion (DF), Toe Extension (EXT), Inversion (INV) • Lateral Compartment • Eversion (EV) • Deep Posterior Compartment • Toe Flexion (flex), Inversion (INV) • Superficial Posterior (Plantar flexion (PF))
Nerves and Blood Supply • Nerves • Sciatic nerve branches into the peroneal (ant/lat) and tibial nerves (post) • Blood Supply • Femoral Artery →Popliteal artery → • Anterior and Posterior Tibial artery • Anterior Tibial becomes the dorsalis pedis artery →dorsal pedal on the dorsum of foot • Posterior Tibial is located behind medial malleolus.
ROM • DF-tibialis anterior, extensor digitorum • PF- gastroc and soleus • INV- tibialis anterior and posteror • EV- peroneals • Toe Ext.-extensor digitorum and hallucis • Toe Flexion flexor digitorum and hallucis
Review • http://www.csuchico.edu/~sbarker/shock/Anklequiz.html • http://www.rad.washington.edu/atlas2/ • http://www.medicalmultimediagroup.com/pated/foot/achilles/achilles.html
Prevention of Injury • Stretch achilles tendon • tight achilles increases risk of plantar fasciitis, achilles tendonitis, and ankle sprains • Strengthen anterior leg muscles • important for shin splints • Strengthen lateral/medial leg muscles • Strengthen intrinsic foot muscles • Good shoes; change shoes, correct type of shoes for playing surface
Injury information • Precursors = something that may predispose an athlete to that injury • All injuries should be treated for symptoms thus RICE. This will not be listed with each injury but should be remembered • HOPS includes information typically seen or heard during the HOPS assessment. Most injuries include swelling, discoloration etc in area, this is not included in slides
Lateral Ankle Sprain • MOI: PF and/or Inv • More common than medial ankle sprains due to (make up about 90% of ankle sprains): • differing length of malleoli (lateral is longer) • Stronger deltoid ligament • Precursors: tight achilles, improper shoes, previous ankle injury • HOPS and Tx • See field strategy 12.2
Medial Ankle Sprain • Less common then lateral ankle sprains • MOI: eversion • Sometimes accompanied by a fracture • HOPS • point tenderness over deltoid and anterior/ posterior joint line • Swelling not as obvious • Takes almost twice as long to recover in some cases
Achilles tendonitis • Precursors: achilles tendon tightness, change in shoes, running surfaces, workout changes • HOPS • chronic injury • pn during and after activity • Thickening of the tendon • Crepitation • Pn with Resistive PF, Passive DF • Tx: stretch achilles, heel lift, tape, ultrasound
Achilles Tendon rupture • Precursors: athletes between 30 and 40, power sports (BB); recreational athletes • HOPT • MOI: push off with knee extending • sharp pain, feels snap or pop • “kicked in the back of the leg” • visible defect/palpable defect • positive Thompson test • Excessive passive DF • Tx: refer to physician
Medial Tibial Stress Syndrome (1) • “shin splints” • Precursors: achilles tendon tightness, change in shoes, running surfaces, workout changes, arch problems • HOPS • sometimes bilateral; pn along distal 1/3 of medial tibial border • initially: pn at start of activity that decreases with activity, then recurring after activity • Later: pain before during and after activity
Medial Tibial Stress Syndrome (2) • HOPS (cont) • Pn increased with AROM PF, INV • Usually responds well to treatment • Tx • Cryotherapy • stretching of achilles • strengthen deep posterior muscle • strengthen anterior muscles
Plantar Fasciitis • Precursors: obesity, achilles tendon tightness, overuse, shoes • HOPT • chronic injury • pn first thing in the morning • point tenderness over the medial calcaneal tubercle • Pn with toe extension and ankle DF • TX- Hot and Cold Modalities, stretching, rest, orthodics, change in shoes, heel lift, tape, roll foot over soda can
Compartment Syndrome (1)“Volkman's Ischemic Contracture” • Two types: • Exertional (MOI:previous injury in leg, chronic onset); Read; **Exertional CS can lead to Acute CS Acute (MOI: blow to front of the leg) • Acute-HOPT • Increasing pain in the front of the leg • firm tight skin in front of shin • loss of sensation between 1st and 2nd toes
Compartment Syn (2) • diminished pulse at dorsalis pedis artery • Inability to DF ankle, or extend toes (progressive) • The 5 Ps (ie, pain, pallor, paresthesias, paralysis, pulselessness) • Tx • Ice and Immobilize • Get to physician (MEDICAL EMERGENCY) • Abnormalities can occur within 30 minutes; irreversible damage can occur within 12-24 hrs
“Turf” Toe • Precursors: hard surfaces, lightweight, flexible shoes, artificial turf • HOPT • MOI-jamming of hallux, hyperextension of toe • sport position requiring hyperextension • Pn, point tnederness over 1st MP joint • Push off phase of running is painful • Pn with passive extension of the great toe • Treatment (TX) • taping, metatarsal pad, stiff soled shoes, manage symptoms
Ingrown toenail • Precursors • improper cutting of toenails, too small shoes, contant sliding of foot in shoes • HOPT • nail grown into the surrounding skin • signs of infection around the nail bed • Tx • See field strategy 12.5
Motron’s Neuroma • Precursors: tight fitting shoes, • HOPT • pn on the plantar side of the foot, usually between the 3rd and 4th metatarsal • Pn and numbness radiates to the 3rd & 4th toes • Pain relieved by Non weight bearing (NWB) • Pn caused by squeezing the foot • Treatment (TX) • taping, metatarsal pad, wider shoes, cortisone shots, surgery
Stress Fractures • Precursors: female athletes with menstrual irregularities (amenorrhea) increase in training regimen, old shoes • common sides: tibia, fibula, neck of 2nd metatarsal • HOPS • pn on WB, relieved by NWB • localized pn (often unilateral) • Tx: complete rest 4-12 weeks, referral for bone scan
Jones Fracture • Avulsion fracture of the peroneus brevis tendon where it attaches to the base of the 5th metatarsal • Common with severe inversion ankle injuries • HOPS: • pn over base of 5th metatarsal • MOI: severe, forceful inversion
Bunions- Hallux Valgus • Medial aspect of 1st MP joint • HOPT • C/S- Shoes, congenital, lig. laxity, prolonged pronation of foot • Angular deformity of the great toe • Pain around the first MP joint (inflammation) • Treatment (TX) • taping, wider shoes, surgery last option
ROM- good/bad; active/passive; perform bilaterally; award a % Strength-good/bad; perform bilaterally; award a % Special Test Thompson Test achilles tendon rupture Anterior Drawer ATF ligament Talar Tilt CF ligament Deltoid ligament Fracture Test- FS 12.6 Tests
Test • Functional Test (p.235-236)- heel raises, walking, balancing, squatting, running, jumping, (progression is the key)
Specialized Rehab • Towel crunches • Theraband Exercises all ROM • Picking up objects (marbles) • BAPS (wobble board) • Stability Trainers • http://www.promedproducts.com/Merchant2/merchant.mv?Screen=CTGY&Store_Code=PP&Category_Code=BB • Achilles Stretch • straight = gastroc • bent = soleus