Download
1 / 10
110 likes | 277 Views
Bladder Continence. Beth Reinke June 16, 2011 SOAR. Urinary Incontinence. Definition: involuntary and unwanted loss of urine. Affects a surprisingly large number of people of all ages.

E N D
Bladder Continence Beth Reinke June 16, 2011 SOAR
Urinary Incontinence • Definition: involuntary and unwanted loss of urine. Affects a surprisingly large number of people of all ages. • Urinary incontinence is the second leading cause of institutionalization of the elderly and seen in over 50% of persons residing in ECFs. • In people living at home the rate may be as high as 53%. • Monetary costs are estimated conservatively at • $28billion • Inability to control urine is one of the most unpleasant and distressing symptoms can individual will can suffer • Commonly causes social isolation, depression and psychological problems. Increases use of indwelling catheters • Associated with problems such as falls, fractures, pressure ulcers UTI’s and depression.
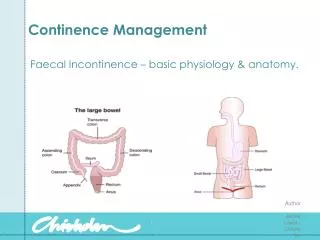
Types of Bladder Dysfunctions • 1. Urinary incontinence • 2. Urinary retention • 3. Urinary tract infections • These conditions can be chronic and in some cases life threatening , a presenting sign of urinary retention is overflow urinary incontinence. A transient cause of incontinence can be either urinary retention or urinary tract infection. Understanding pathophysiology of the bladder is essential
Types • Transient incontinence- DRIP • Urge incontinence • Stress urinary incontinence • Mixed incontinence • Overflow incontinence • Functional urinary incontinence
Other interventions to control incontinence • Pelvic Muscle Exercises • Biofeedback • Electrical Stimulation • Intermittent Self catheterization • Urinary clamps • Pharmacological Treatment of incontinence • Surgical Treatments • Indwelling catheters, external catheters • Containment- diapers, pads.
Urinary Tract Infections Catheter associated urinary tract infections (CAUTI) are one of the most frequent infections today. The daily risk of developing CAUTI is 3-7% in acute care. The centers for Medicare and Medicaid services (CMS) identified hospital acquired CAUTI as one of 8 conditions for which hospitals will not receive additional reimbursement. Long-term facilities also follow CMS regulatory guidance. Use of catheters must be medically justified and care rendered to reduce the risk of complications
Risks of CAUTI • Cystitis, periurethral abscess, prostatitis, epididymitis, and acute or chronic pyelonephritis • Gram negative bacteremia • Urosepsis which can be fatal in 40-60%
The DX of CAUTI is based on finding bacteriuria, along with elevated WBC on a urinalysis examination. Additional, in some cases, an elevated serum WBC and 2 or more of the following S/S • Pain or burning in the region of the bladder, urethra, or flank • Fever greater than 100.4 or chills • Malaise • Offensive urine odor • Change of color or character of urine, including cloudy urine of increased sediment • Hematuria • Bladder spasms/leakage • Catheter obstruction • Increased weakness or spasticity especially in those with neurologica disease or injury • Change in mental status, esp in older adults ie confusion, lethargy, agitation, delirium, or subtle changes in behavior • Bacteremia Prevention of CAUTI Sterile Smallest catheter lumen, balloon Minimal duration, closed drainage system Bag below the level of bladder Routine perineal care Measures to prevent tension or traction on the catheter. Increasing fluid intake may be of some benefit
Summary: • Urinary and fecal incontinence are underreported problems. • In many instances, minimally invasive nursing interventions may lessen or treat the incontinence. • If those interventions are not successful- it is important to obtain referrals to obtain more information or appropriate testing to determine the problem and perhaps alleviate or reverse the debilitation consequences of incontinence.