Download
1 / 24
310 likes | 829 Views
Ketamine Bladder. Carmel Ramage 19 th October 2012. Case Presentation. 24 year old woman Complaining of Urinary frequency Urgency Pain Dysuria - shooting and leads to poor flow because tenses up post micturation pain Symptoms of recurrent UTI but one proven UTI

E N D
Ketamine Bladder Carmel Ramage 19th October 2012
Case Presentation • 24 year old woman • Complaining of • Urinary frequency • Urgency • Pain • Dysuria - shooting and leads to poor flow because tenses up • post micturation pain • Symptoms of recurrent UTI but one proven UTI • Jelly like urethral discharge • Deep dyspareunia
History • P 1+4 • No significant medical history • Smoker • Social alcohol intake • NKDA • 10 stone – lost weight but normal appetite • LFT – only raised gamma GT
Examination • Pelvic examination – normal • Urethra –no discharge • Attempted cystoscopy in OPD – very tender and in severe discomfort • Cystoscopy under GA
Cystoscopy • Severe haematuria • Unable to visualise any anatomy • No response to saline washout • Indwelling catheter left in situ • USS organised
Further investigations • USS – fluid in POD, catheter in bladder • Discussed with Urologists • CT recommended • Free fluid confirmed in pelvis and abdomen • Bladder abnormally thick walled and small • Plan • Catheter in for 2 weeks • Cystogram
Diagnosis • Re-interviewed following initial USS and CT • Admitted to Ketamine use for 4 years • Several times a week for a year • Stopped during pregnancy (2008) • Now once / twice monthly • Previous hospital admission (November 2010) with severe abdominal pain following sniffing ketamine • Managed conservatively • Treated for UTI • Readmission 4 months later with upper abdominal pain • Gastroscopy ) • Abdominal USS ) NAD • Renal USS )
Cystogram • Small volume bladder (20mls) and patient unable to tolerate • CT • No further fluid in pelvis and abdomen • contrast in uterus and vagina – suspicion of vesico-uterine fistula • Repeat cystogram 3 weeks later • Severe pain on distending bladder • No extravasation seen
Ongoing Management • Continued with indwelling catheter • Started on Solifenacin • Cystistat bladder installations • Aware that symptoms may not settle due to irreversible bladder fibrosis • May need Augmentation cystoplasty
Current Update • Cystistat bladder instillations for 8 months • Symptoms • Daytime frequency – 3 hourly • Nightime – 6 hourly • Full bladder without urgency • No bladder pain • No Haematuria • No UTI • No need for reconstructive bladder surgery
Ketamine • Fastest growing "party drug" among 16-24 year olds • Also known as • Special K • Kit-Kat • Ket • Cat valium • Vitamin K • Estimated 125,000 users in the UK • More users than crack and heroin combined in UK and Wales
History • Developed by Parke-Davis in 1962 • First given to American soldiers during the Vietnam War • Battlefield / emergency anaesthetic • Short duration of action • Dissociative anaesthesia • Muscle paralysis • Increase in illicit use in USA during 1990’s • Class C drug (January 2006) • Possession - 2 years • Supply - 14 years • Unlimited fine
Ketamine effects • Floating feeling • may feel completely detached from body and surroundings • Dissociative paralysis – “entering the K-hole” • Change in perception • Hallucinations • ‘Trip’ for up to an hour • After effects may take several hours to wear off • Confusion • Panic attacks • Depression • Exacerbation of any pre-existing mental health problems
Ketamine Use • Sold in either powdered or liquid form • Inhaled as snuff • Injected • Orally • Bitter taste • Slower onset of action • Ecstasy Tablets known as "Strawberry“ and "Sitting Duck" contained Ketamine • >80% ketamine seized in the US is of Mexican origin
Ketamine Detection • Urine • Blood/ plasma • Norketamine • Pharmacologically-active metabolite • Plasma levels: • Therapeutic - 0.5-5.0 mg/L • Arrested for impaired driving – 1–2 mg/L • Acute fatal overdose - 3–20 mg/L
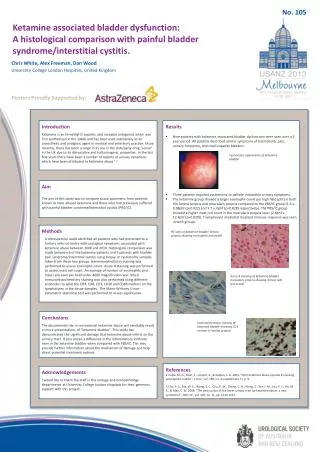
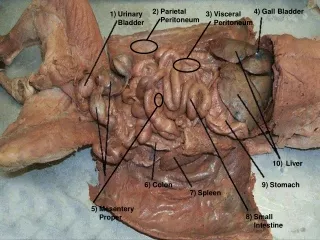
Ketamine and Urinary system • “Bristol bladder” • described in 20081 • frequency, haematuria, incontinence and dysuria associated with ketamine use* • Scarred thickened shrunken bladder • Erythema with contact bleeding • Severe ulcerative cystitis • Can ascend to ureters and kidneys • Symptomatic relief • Cessation of Ketamine use2 • PentosanPolysulphate 1Cottrell et al 2008. BMJ 336: 973 2Shahani et al 2007 Urology 69 (5)
Presentation • “K cramps” • Severe long lasting abdominal pain • Cause unknown • Usually limited to users of >1 g / day • Hepatic damage • Urinary tract • Overactive bladder syndrome • Painful bladder symptoms • Incontinence • Upper tract obstruction • Renal papillary necrosis • Patients erroneously treated for recurrent UTI’s/ painful bladder syndrome
Ketamine and Bladder damage • Causal link • Precise mechanism unclear • Direct toxicity of Ketamine or its metabolites (supported by animal models) • Microvascular damage • Autoimmune reaction triggered by circulating or urinary ketamine • Unrecognised bacteruria • Toxicity receptor mediated • No NDMA receptors in bladder
Diagnosis of Ketamine Bladder • Cystoscopy • Denuded urothelium • Can slough off as intact sheets of cells • Histology • Absence of urothelium • Eosinophilia in blood vessels • Lymphocytic infiltration • mast cells • Cell Markers • P53 (assoc. with cell death)– high • Ki07 (assoc. with cell growth) - very low • CK20 (assoc with Ca in situ)– absent Wood et al 2011; BJUI 107:1881-1884
How to make the Diagnosis • Good history of recreational drug abuse • MSU for C&S • Cystoscopy and biopsy • Renal function tests • CT urogram for extent of disease
Treatment • Stop ketamine • Involve • drug support agencies • GP • National Club Drug Clinic London (Chelsea and Westminister) • Liaise with chronic pain team • Medication • Bupenorphine patches • Co-codamol • Amytriptyllineat night (Bristol) • Anticholinergics • Intra-vesicalinstallations • Bladder augmentation / urinary diversion +/- cystectomy
Future • Awareness and Education of Clinical Staff • Education and Support for ketamine users • Effects on the urinary tract • Where to seek help • Liaison with pain services, psychiatry, social services
Summary • Increasing Ketamine use • May cause significant urinary tract damage • Be aware of potential diagnosis in young patients with severe painful bladders