Download
1 / 1
10 likes | 176 Views
Social Well-being Predictors of Positive Mental Health in the Irish Adult Population. Van Lente, E. 1 , Barry, M. M. 1 , Molcho M. 1, on behalf of the SLÁN 2007 consortium 2 Health Promotion Research Centre, Department of Health Promotion, National University of Ireland, Galway

E N D
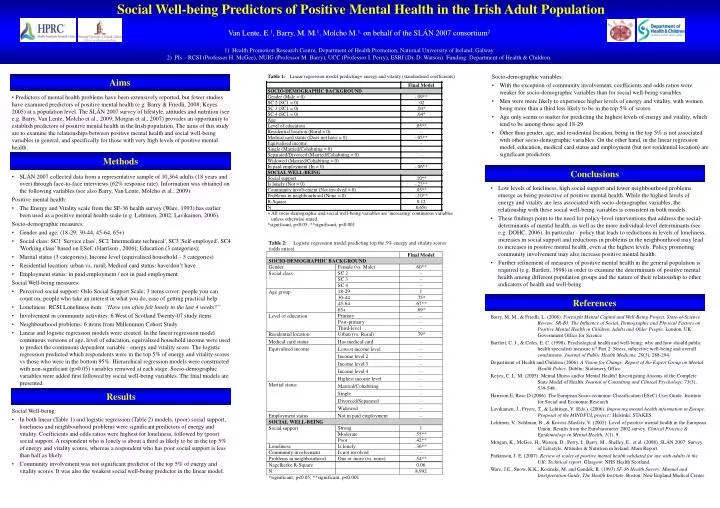
Social Well-being Predictors of Positive Mental Health in the Irish Adult Population • Van Lente, E.1, Barry, M. M.1, Molcho M.1, on behalf of the SLÁN 2007 consortium2 • Health Promotion Research Centre, Department of Health Promotion, National University of Ireland, Galway • PIs – RCSI (Professor H. McGee), NUIG (Professor M. Barry), UCC (Professor I. Perry), ESRI (Dr. D. Watson). Funding: Department of Health & Children. Socio-demographic variables: • With the exception of community involvement, coefficients and odds ratios were weaker for socio-demographic variables than for social well-being variables. • Men were more likely to experience higher levels of energy and vitality, with women being more than a third less likely to be in the top 5% of scores. • Age only seems to matter for predicting the highest levels of energy and vitality, which tend to be among those aged 18-29. • Other than gender, age, and residential location, being in the top 5% is not associated with other socio-demographic variables. On the other hand, in the linear regression model, education, medical card status and employment (but not residential location) are significant predictors. Aims • Predictors of mental health problems have been extensively reported, but fewer studies have examined predictors of positive mental health (e.g. Barry & Friedli, 2008; Keyes 2005) at a population level. The SLÁN 2007 survey of lifestyle, attitudes and nutrition (see e.g. Barry, Van Lente, Molcho et al., 2009; Morgan et al., 2007) provides an opportunity to establish predictors of positive mental health in the Irish population. The aims of this study are to examine the relationships between positive mental health and social well-being variables in general, and specifically for those with very high levels of positive mental health. Methods Conclusions • SLÁN 2007 collected data from a representative sample of 10,364 adults (18 years and over) through face-to-face interviews (62% response rate). Information was obtained on the following variables (see also Barry, Van Lente, Molcho et al., 2009): Positive mental health: • The Energy and Vitality scale from the SF-36 health survey (Ware, 1993) has earlier been used as a positive mental health scale (e.g. Lehtinen, 2002; Lavikainen, 2006). Socio-demographic measures: • Gender and age: (18-29, 30-44, 45-64, 65+) • Social class: SC1 'Service class', SC2 'Intermediate technical', SC3 'Self-employed', SC4 'Working class’ based on ESeC (Harrison , 2006); Education (3 categories); • Marital status (3 categories); Income level (equivalised household – 5 categories) • Residential location: urban vs. rural; Medical card status: have/don’t have • Employment status: in paid employment / not in paid employment Social Well-being measures: • Perceived social support: Oslo Social Support Scale; 3 items cover: people you can count on, people who take an interest in what you do, ease of getting practical help • Loneliness: RCSI Loneliness item: “Have you often felt lonely in the last 4 weeks?” • Involvement in community activities: 6 West of Scotland Twenty-07 study items • Neighbourhood problems: 6 items from Millennium Cohort Study • Linear and logistic regression models were created. In the linear regression model continuous versions of age, level of education, equivalized household income were used to predict the continuous dependent variable - energy and vitality score. The logistic regression predicted which respondents were in the top 5% of energy and vitality scores vs those who were in the bottom 95%. Hierarchical regression models were constructed with non-significant (p>0.05) variables removed at each stage. Socio-demographic variables were added first followed by social well-being variables. The final models are presented. • Low levels of loneliness, high social support and fewer neighbourhood problems emerge as being protective of positive mental health. While the highest levels of energy and vitality are less associated with socio-demographic variables, the relationship with these social well-being variables is consistent in both models. • These findings point to the need for policy-level interventions that address the social-determinants of mental health, as well as the more individual-level determinants (see e.g. DOHC, 2006). In particular - policy that leads to reductions in levels of loneliness, increases in social support and reductions in problems in the neighbourhood may lead to increases in positive mental health, even at the highest levels. Policy promoting community involvement may also increase positive mental health. • Further refinement of measures of positive mental health in the general population is required (e.g. Bartlett, 1998) in order to examine the determinants of positive mental health among different population groups and the nature of their relationship to other indicators of health and well-being. References Barry, M. M., & Friedli, L. (2008). Foresight Mental Capital and Well-Being Project.State-of-Science Review: SR-B3. The Influence of Social, Demographic and Physical Factors on Positive Mental Health in Children, Adults and Older People. London, UK: Government Office for Science Bartlett, C. J., & Coles, E. C. (1998). Psychological health and well-being: why and how should public health specialists measure it? Part 2: Stress, subjective well-being and overall conclusions. Journal of Public Health Medicine, 20(3), 288-294. Department of Health and Children (2006). A Vision for Change: Report of the Expert Group on Mental Health Policy. Dublin: Stationery Office. Keyes, C. L. M. (2005). Mental Illness and/or Mental Health? Investigating Axioms of the Complete State Model of Health. Journal of Consulting and Clinical Psychology, 73(3), 539-548. Harrison E, Rose D (2006). The European Socio-economic Classification (ESeC) User Guide. Institute for Social and Economic Research Lavikainen, J., Fryers, T., & Lehtinen, V. (Eds.). (2006). Improving mental health information in Europe. Proposal of the MINDFUL project.: Helsinki: STAKES. Lehtinen, V., Sohlman, B., & Kovess-Masfety, V. (2005). Level of positive mental health in the European Union: Results from the Eurobarometer 2002 survey. Clinical Practice & Epidemiology in Mental Health, 1(1), 9. Morgan, K., McGee, H., Watson, D., Perry, I., Barry, M., Shelley, E., et al. (2008). SLÁN 2007: Survey of Lifestyle, Attitudes & Nutrition in Ireland. Main Report. Parkinson, J. E. (2007). Review of scales of positive mental health validated for use with adults in the UK: Technical report. Glasgow: NHS Health Scotland. Ware, J.E., Snow, K.K., Kosinski, M. and Gandek, B. (1993) SF-36 Health Survey: Manual and Interpretation Guide, The Health Institute. Boston: New England Medical Center. Results Social Well-being: • In both linear (Table 1) and logistic regression (Table 2) models, (poor) social support, loneliness and neighbourhood problems were significant predictors of energy and vitality. Coefficients and odds ratios were highest for loneliness, followed by (poor) social support. A respondent who is lonely is about a third as likely to be in the top 5% of energy and vitality scores, whereas a respondent who has poor social support is less than half as likely. • Community involvement was not significant predictor of the top 5% of energy and vitality scores. It was also the weakest social well-being predictor in the linear model.