Download
1 / 30
370 likes | 728 Views
Dyslexia: A Specific Learning Disability in Reading. Dr. Robert Isherwood 121 High Incidence Disabilities Fall 2011. Class Objectives:. TLW identify characteristics of dyslexia TLW engage in a reading activity to simulate dyslexia

E N D
Dyslexia: A Specific Learning Disability in Reading Dr. Robert Isherwood 121 High Incidence Disabilities Fall 2011
Class Objectives: • TLW identify characteristics of dyslexia • TLW engage in a reading activity to simulate dyslexia • TLW analyze the importance of the grapheme phoneme relationship
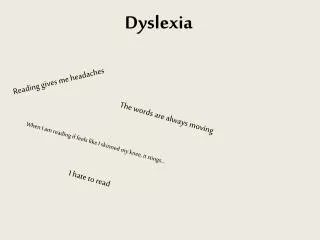
What is dyslexia? • Dyslexia is a specific learning disability that is neurological in origin. It is characterized by difficulties with accurate and/or fluent word recognition and by poor spelling and decoding abilities. These difficulties typically result from a deficit in the phonological component of language that is often unexpected in relation to other cognitive abilities and the provision of effective classroom instruction. Secondary consequences may include problems in reading comprehension and reduced reading experience that can impede the growth of vocabulary and background knowledge.
Dyslexia (cont.) • Neuroscientific research indicates that dyslexia has a genetic basis • Some people with dyslexia have a different anatomical brain structure • Functional magnetic resonance imaging studies indicate difference in brain processing between individuals with dyslexia from those without dyslexia
What is Dyslexia? • Dyslexia- an inability to distinguish or separate the sounds in spoken words • Children with dyslexia usually have problems with reading, spelling, writing, and sometimes numbers • Problems coping with written symbols • May have organizational problems, problems with left and right, and following instructions • Dyslexia affects about 2% to 8% of school age children
What causes Dyslexia? • The exact causes of dyslexia are still not completely clear, but anatomical and brain imagery studies show differences in the way the brain of a dyslexic person develops and functions. • Moreover, most people with dyslexia have been found to have problems with identifying the separate speech sounds within a word and/or learning how letters represent those sounds, a key factor in their reading difficulties. • Dyslexia is not due to either lack of intelligence or desire to learn; with appropriate teaching methods, dyslexics can learn successfully.
Dyslexia (cont.) • Neuroscientific research indicates that dyslexia has a genetic basis • Some people with dyslexia have a different anatomical brain structure • Functional magnetic resonance imaging studies indicate difference in brain processing between individuals with dyslexia from those without dyslexia
Parts of brain associated with reading Broca’s area is named after French neurosurgeon Paul Broca. He discovered the left inferior area of the frontal cortex has a tremendous role in the process of language. German neurologist Carl Wernicke located an area in the posterior section of the left temporal lobe that is responsible for processing words we hear.
The Neural Loop of Reading Neuroscientists now agree that running around the lateral sulcus (also known as the fissure of Sylvius) in the left hemisphere of the brain, there is a sort of neural loop that is involved both in understanding and in producing spoken language. At the frontal end of this loop lies Broca's area, which is usually associated with the production of language, or language outputs . At the other end (more specifically, in the superior posterior temporal lobe), lies Wernicke's area, which is associated with the processing of words that we hear being spoken, or language inputs. Broca's area and Wernicke's area are connected by a large bundle of nerve fibres called the arcuate fasciculus http://www.youtube.com/watch?v=XKekE10b82s&feature=related
Grapheme-Phoneme Correspondence • Relationship between speech sound (phoneme) and written symbol (grapheme).
What is strephosymbolia? • Once called Word Blindness • a learning disorder in which symbols and especially phrases, words, or letters appear to be reversed or transposed in reading • Term was coined by Dr. Samuel Orton • Occurs in only 5% of dyslexics
Areas of Cognitive Weakness • Difficulties with phonemic awareness • Problems with word retrieval or rapid automatic naming (automaticity) • Poor digit span • Difficultly with sequencing or ordering • Visual perception confusion • http://www.youtube.com/watch?v=g6NiD1GchJc&feature=related
You can go from corner A to corner B by climbing the stairs or by going around a level plane.
The rows of black and white squares are all parallel.The vertical zigzag patterns disrupt our horizontal perception
Three-prong fork and two sticks?.Incongruous design elements on opposite ends of the parallel lines create confusion.
Let’s do some reading activites: • Read “ A Fairy Tale” out loud to a partner • Discuss with your partner what fairy tale you think you were attempting to read • What problems did you encounter? • Next, read “The Highty Marfus” to yourself • Sit with your partner and attempt to answer the comprehension questions • What is the point of the exercise?????
Early Signs of Dyslexia • Symptoms of dyslexia are variable depending on the child and his/her surroundings • Early diagnosis is difficult until the child is at the age at which reading typically begins (age 6) • Jumbling sounds or words in speech • Confusing words signifying direction in space (up/down, in/out, etc.) • Delayed speech development • Difficulty with behavior and low frustration level • Difficulty getting dressed, buttoning, tying shoes • Difficulty hopping, skipping, throwing, catching
Common Myths about Dyslexia • A person can grow out of dyslexia • Poor schooling or poverty can cause dyslexia • All children with dyslexia sees letters and symbols up side down or inversely • ADHD can cause dyslexia • Dyslexia can be cured • People with dyslexia are destined for a life of failure and will never learn to read
How do we assess for a SLD? • Discrepancy Model • RtII Model- Response to Intervention and Instruction • Neither model is required by the IDEA. However, schools must choose one of the methods to determine if a child has a SLD
Discrepancy Model • The IQ-achievement discrepancy model assesses whether there is a significant difference between a student’s scores on a test of general intelligence (e.g., an IQ test such as the WISC-IV) and scores obtained on an achievement test (e.g., the Woodcock Johnson Achievement Test). The IQ-achievement discrepancy model is the approach traditionally used to identify children with learning disabilities.
Example of the Discrepancy Model If a student’s score on the IQ test is at least two standard deviations (30 points) higher than his or her scores on an achievement test, the student is described as having a significant discrepancy between IQ and achievement and, therefore, as having a learning disability.
Standard Score Less than 70 70-79 80-89 90-109 110-119 120-129 130 and higher Classification Development. Delay Borderline MR Low Average Average High Average Superior Very Superior Standard Score
An example problem: • John is a student struggling with academics in second grade. He is referred for an evaluation and the school psychologist gives him the Stanford-Binet IQ test. John receives a FSIQ of 96. He is then given the WIAT and earns a standard score of 48 on the reading comprehension sub-test, an 88 on the math problem solving subtest, and a 77 on the vocabulary subtest. Does he have a SLD? Tell me why!
Criticism of the Discrepancy Model • This method does not allow schools to identify children as having learning disabilities while they are still in the primary grades. • Students often struggle for years prior to being identified as having learning disabilities. • Students often do not receive the support they need in the early grades. • The information gathered from the IQ and achievement assessments does not indicate each student’s specific learning needs: • The assessment process does little to inform classroom instruction. • Has been called the “Wait and Fail Model”
Defining RtII • Response to Intervention (RtI) is a systematic decision-making process designed to allow for early and effective responses to children’s learning and behavioral difficulties, provide children with a level of instructional intensity matched to their level of need and then provide a data-based method for evaluating the effectiveness of instructional approaches. RtI relies on evidence-based instructional practices and frequent progress monitoring to provide the data necessary to make decisions about child progress and the need for more intensive intervention. The model is intended to reduce unnecessary referrals to special education. • http://www.youtube.com/watch?v=IsAqh2Pxg0A