Download
1 / 66
660 likes | 784 Views
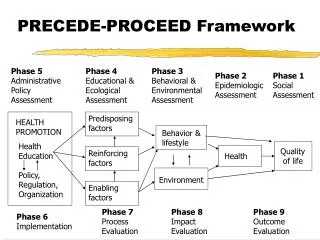
Cardiology. For Phase 1a Maria Digby & Rowena Speak. The Peer Teaching Society is not liable for false or misleading information…. What we’re going to cover…. 1 st Half Physiology Pharmacology Anatomy ECG 2 nd Half Pathophysiology + Clinical Scenarios More Pharmacology!

E N D
Cardiology For Phase 1a Maria Digby & Rowena Speak The Peer Teaching Society is not liable for false or misleading information…
What we’re going to cover… 1st Half • Physiology • Pharmacology • Anatomy • ECG 2nd Half • Pathophysiology + Clinical Scenarios • More Pharmacology! • Question time The Peer Teaching Society is not liable for false or misleading information…
Ventricles • Phase 0: depolarisation – Na+ in • Phase 1: partial repolarisation – Na+ channels shut, K+ out • Phase 2: plateau – Ca2+ in through L-type channels • Phase 3: repolarisation – K+ out • Phase 4: resting potential – (-90mV) – Na+/K+ ATPase The Peer Teaching Society is not liable for false or misleading information…
SAN • Phase 4 = pacemaker potential – less K+ out, Na+ in through F-type channels, Ca2+ in through T-type channels • Phase 0 = slower depolarisation – Ca2+ in through L-channels NOT Na+ in like depolarisation ventricles!) • Phase 3 = repolarisation – K+ out The Peer Teaching Society is not liable for false or misleading information…
Antiarrhythmic drugs: Vaughan Williams classification • Class I: Na+ channel blockers 1a) Quinidine – moderate blocker 1b) Lignocaine – weak blocker 1c) Flecainide – strong blocker • Class II: Beta blockers: block sympathetic stimulation - atenolol • Class III: K+ channel blockers: prolong repolarisation - amiodarone • Class IV: Ca2+ channel blockers: verapramil Phase 1 IV Phase 2 0 mV III I Phase 0 Phase 3 -80mV Phase 4 II The Peer Teaching Society is not liable for false or misleading information…
Cardiac cycle • AP = aortic pressure • LVP = left ventricular pressure • LAP = left atrial pressure • LVEDV = left ventricular end diastolic volume • LVESV = left ventricular end systolic volume The Peer Teaching Society is not liable for false or misleading information…
Cardiac cycle: Systole • Systole • After ventricular filling, pressure in ventricles > in atria = AV valves close (SOUND 1 = “lub”) • Isovolumetric contraction: ventricles contracts when all valves are shut (this increases pressure in ventricles) • Ventricular ejection: pressure in ventricles > in pulmonary artery/aorta = semilunar valves open and blood flows out of ventricle The Peer Teaching Society is not liable for false or misleading information…
Cardiac cycle: Diastole • Diasystole • After ventricular ejection, pressure in pulmonary artery/aorta > than in ventricles = semilunar valves shut (SOUND 2 = “dub”) • Isovolumetric relaxation: ventricles relax when all valves are shut (this decreases the pressure in the ventricles) • Ventricular filling: pressure in ventricles < in atria = AV valves open The Peer Teaching Society is not liable for false or misleading information…
Cardiac cycle: “atrial kick” • Ventricular filling is mostly a passive process • But towards the end of diastole, the atria contract causing a small increase in pressure in the ventricles = “atrial kick” The Peer Teaching Society is not liable for false or misleading information…
Cardiac cycle: dicrotic notch • When the aortic valve closes, blood rebounds against the valve causing a decrease then a rebound of aortic pressure = dicrotic notch The Peer Teaching Society is not liable for false or misleading information…
Equations: learn these!! • SV = EDV - ESV • CO = HR x SV • MAP = DP + 1/3(SP-DP) • BP = CO x TPR The Peer Teaching Society is not liable for false or misleading information…
Monitoring MAP: Baroreceptors Where are the arterial baroreceptors? a) Carotid sinus + b) Aortic arch • Baroreceptors detect changes in arterial pressure • Afferent nerve (Glossopharyngeal) • CNS (Medullary Cardiovascular Centre) • Efferent nerve • Sympathetic outflow to heart and arterioles • Parasympathetic (Vagus) outflow to heart The Peer Teaching Society is not liable for false or misleading information…
Maintaining MAP (BP = CO x TPR) CO TPR BP The Peer Teaching Society is not liable for false or misleading information…
Maintaining MAP: 1. Changing CO • CO = HR x SV • Change Heart Rate • Sympathetic nervous stimulation of the heart • Parasympathetic nervous stimulation of the heart (Vagus) • Plasma adrenaline • Change Stroke Volume • Sympathetic nervous stimulation of the heart • Plasma adrenaline • End-diastolic ventricular volume (preload) – FRANK-STARLING MECHANISM The Peer Teaching Society is not liable for false or misleading information…
FRANK-STARLING MECHANISM – learn this! At any given heart rate…. Any ↑ Venous Return…. Causes ↑ End-Diastolic Volume… Causes ↑ stretch in the cardiac muscle (Preload)… Causes ↑ forceful contraction… Which ↑ Stroke Volume and thereby the Cardiac Output The Peer Teaching Society is not liable for false or misleading information…
Maintaining MAP: 2. Changing TPR • The arterioles are the principle site of resistance to blood flow • Vasoconstriction • Local: Endothelin-1, internal blood pressure (myogenic response) • Neural: Sympathetic nerves • Hormonal: Adrenaline (on alpha receptors), Angiotensin II, Vasopressin (aka Antidiuretic hormone) • Vasodilation • Local: decrease in Oxygen, increase in CO2/H+, Nitric Oxide, Eicosanoids, Prostacyclin • Neural: Neurons that release Nitric oxide • Hormonal: Adrenaline (on beta 2 receptors), Atrial Natriuretic Peptide The Peer Teaching Society is not liable for false or misleading information…
Important point… • There is sympathetic stimulation to both the heart and arterioles • But there is no parasympathetic stimulation to the arterioles, only to the heart The Peer Teaching Society is not liable for false or misleading information…
Terms to understand… • Active hyperaemia – vasodilation in response to an increase in metabolic activity • Flow autoregulation – vasodilation in response to decreased pressure • Reactive hyperaemia – when a tissue’s blood supply has been completely occluded, on removal of the occlusion there is a profound, transient increase in blood flow The Peer Teaching Society is not liable for false or misleading information…
GO LOOK AT… • VANDERS - especially page 399 (12th edition) The Peer Teaching Society is not liable for false or misleading information…
Long term regulation of MAP • The Baroreceptor reflex is a short term regulator. They end up adapting to a maintained change in pressure. • The most important long-term regulator of arterial pressure is blood volume – this is regulated by the Renin-Angiotensin-Aldosterone System (RAAS) • ACE inhibitors inhibit RAAS to reduce blood volume (have a quick look at RAAS – try to understand it but don’t worry about memorising it until Phase 1b!) The Peer Teaching Society is not liable for false or misleading information…
RAAS The Peer Teaching Society is not liable for false or misleading information…
Haemostasis • Platelet plug • Clotting cascade • Clotting factors dependent upon Vitamin K: II, VII, IX, X • Haven’t got time to talk about this now – make sure you understand the principles of it • Important for understanding pharmacology of Aspirin, Clopidogrel, Warfarin, Heparin and Fibrinolytics The Peer Teaching Society is not liable for false or misleading information…
Anatomy - valves The Peer Teaching Society is not liable for false or misleading information…
Anatomy - valves The Peer Teaching Society is not liable for false or misleading information…
Valve pathology The Peer Teaching Society is not liable for false or misleading information…
Rheumatic fever • Endocarditis • Post-Streptococcus pyogenes infection • (Scarlet fever, Strep throat) • Damages heart valves The Peer Teaching Society is not liable for false or misleading information…
Anatomy – heart borders Right: formed by right atrium, runs between 3rd and 6th right costal cartilages approximately 2-3cm from the midline in the adult Left: formed by left atrial appendage + left ventricle, apex 2nd left intercostal space 2-3cm from midline Inferior: formed by right atrium and right ventricle + tiny bit of left ventricle The Peer Teaching Society is not liable for false or misleading information…
Anatomy – aorta • Thoracic • Right + left coronary arteries • Brachiocephalic (aka innominate) artery • Left common carotid artery • Left subclavian artery • Passes through diaphragm at T12 • Abdominal • Abdominal aortic aneurysm – expansile, pulsatile mass, midline, above umbilicus • Bifurcates at L4 The Peer Teaching Society is not liable for false or misleading information…
Electrocardiography (ECG) – heart rate • HeartRate • Quick estimation = 10 x no. of QRS complexes on one rhythm strip (check speed of ECG is 25mm/s) • Sinus bradycardia < 60bpm • Sinus tachycardia >100bpm • Normal PR interval = 0.12-0.20s • Normal QRS complex = 0.08-0.12s The Peer Teaching Society is not liable for false or misleading information…
ECG – AV block • 1st degree – PR interval prolonged, >0.20sec • 2nd degree:- • Mobitz type I - progressive lengthening of PR interval with each successive complex until a P wave is not conducted • Mobitz type II – PR interval constant, QRS complexes dropped intermittently or in fixed ratio to P wave rate • 3rd degree - Complete dissociation of P Waves and QRS complexes The Peer Teaching Society is not liable for false or misleading information…
ECG • Atrial flutter = saw tooth pattern • Atrial fibrillation = irregularly irregular rhythm The Peer Teaching Society is not liable for false or misleading information…
ECG – Ventricular fibrillation: fine and coarse • Ventricular fibrillation The Peer Teaching Society is not liable for false or misleading information…
Useful websites • http://www.cvphysiology.com • http://www.cvpharmacology.com/ The Peer Teaching Society is not liable for false or misleading information…
Pathology/Pathophysiology • Normal arterial structure The Peer Teaching Society is not liable for false or misleading information…
Getting old ain’t pleasant • Progressive fibrous thickening of intima • Fibrosis + scarring of muscular or elastic media • Accumulation of mucopolysaccharide-rich ground substance • Fragmentation of elastic laminae • ATHEROSCLEROSIS The Peer Teaching Society is not liable for false or misleading information…
Atherosclerosis • Some predisposing factors? • Prevented? The Peer Teaching Society is not liable for false or misleading information…
Atherosclerosis • Effects medium and large arteries Risk factors: • Aging • Male • Hypertension • Smoking • Diabetes mellitus • Hyperlipidemia • Increase LDL • Decreased HDL • Having a factor 7 genetics • Lifestyle • Exercise • Obesity • Diet • Stress and personality The Peer Teaching Society is not liable for false or misleading information…
Drugs – ‘all’s well that ends well’ ;) • Drugs • Calcium channel blockers “ipine”seg: amlodipine • ACE Inhibitors “il”seg: ramipril • Angiotensin Receptor Blockers “sartans” eg: candesartan • Diuretics “ide”seg: loop – furosemide, thiazide – bendoflumethiazide and K sparing - Amiloride • Beta blockers “olol”seg: atenolol • Statins “statin”eg: simvastatin The Peer Teaching Society is not liable for false or misleading information…
Clopidogrel - is an oral, thienopyridine class antiplatelet agent • Anticoagulants “rin”eg: warfarin and heparin • NSAIDS “profen” eg: ibuprofen, aspirin *so doesn’t work for everything The Peer Teaching Society is not liable for false or misleading information…
The Peer Teaching Society is not liable for false or misleading information…
Angina Pectoralis • Caused by chronic heart disease • Atherosclerosis in the coronary artery • Means less O2 to heart muscle • Crushing chest pain • No troponin • No new changes on ECG • Stable or unstable? • Stable - Caused by activity / stress (watching Barnsley) - relieved by GTN/rest • Unstable - NOT relieved by GTN /rest - Can occur at rest The Peer Teaching Society is not liable for false or misleading information…
MI What is an MI? How does it occur? How does it present? How is it prevented? • ST elevation myocardial infarction • Non-STelevation myocardial infarction The Peer Teaching Society is not liable for false or misleading information…
MI - STEMI • Crushing chest pain • Feeling of “impending doom” in Barnsley – “gonna miss Barnsley play at weekend” ;) • Nausea • Sweating • SOB • Clammy skin • Raised Troponin level • ST elevation on ECG The Peer Teaching Society is not liable for false or misleading information…
MI - STEMI • STEMI • Ambulance • MONA • A and E • β blocker (atenolol) • Thrombolytics (tPA or streptokinase) • ACE inhibitor (lisinopril) • Clopidogrel • Back at home • Warfarin • Aspirin • βBlocker (metoprolol) • ACE inhibitor • Statin (simvastatin) The Peer Teaching Society is not liable for false or misleading information…
MI - NSTEMI • Infarct • Feeling again same “impending doom” - Barnsley be relegated? • Nausea • Sweating • SOB • Clammy skin • Raised Troponin • No new ECG changes The Peer Teaching Society is not liable for false or misleading information…
MI - NSTEMI NSTEMI Ambulance • MONA • M= Morphine • O = Oxygen • N = Nitrates • A = Aspirin A and E • βblocker (atenolol) • LMW heparin • GPIIb/IIIa antagonist (tirofiban) • Nitrates • Clopidogrel Back at home • Warfarin • Aspirin • βBlocker (metoprolol) • ACE inhibitor • Statin The Peer Teaching Society is not liable for false or misleading information…
Heart Failure • Heart failure = pathophysiological state in which the heart is unable to pump sufficient blood to meet the needs of the metabolising tissues or can only do so with elevated filling pressures • R, L or Congestive • Systolic / diastolic /Both • Excessive salt and water retention • Low cardiac output and raised peripheral resistance The Peer Teaching Society is not liable for false or misleading information…
Causes:- • Ischaemic heart disease – 34% • Dilated cardiomyopathy – 32% • Primary valvular disease and congenital heart disease – 12% • Hypertensive heart disease – 11% • Other -5% The Peer Teaching Society is not liable for false or misleading information…
Physiological • A state where the heart is unable to pump enough blood to satisfy the needs of the metabolising tissues • Clinical • A symptomatic condition where breathlessness, tiredness and fatigue are associated with a cardiac abnormality that reduces cardiac output The Peer Teaching Society is not liable for false or misleading information…
Key concepts - Pathophysiology • Initial insult • Fall in cardiac output • ↑Preload to maintain ventricular performance • ↑Afterload limits ventricular performance • Maladaptive hormonal responses • Progressive left ventricular remodelling • Progressive decline in cardiac performance The Peer Teaching Society is not liable for false or misleading information…