Download
1 / 24
240 likes | 1.08k Views
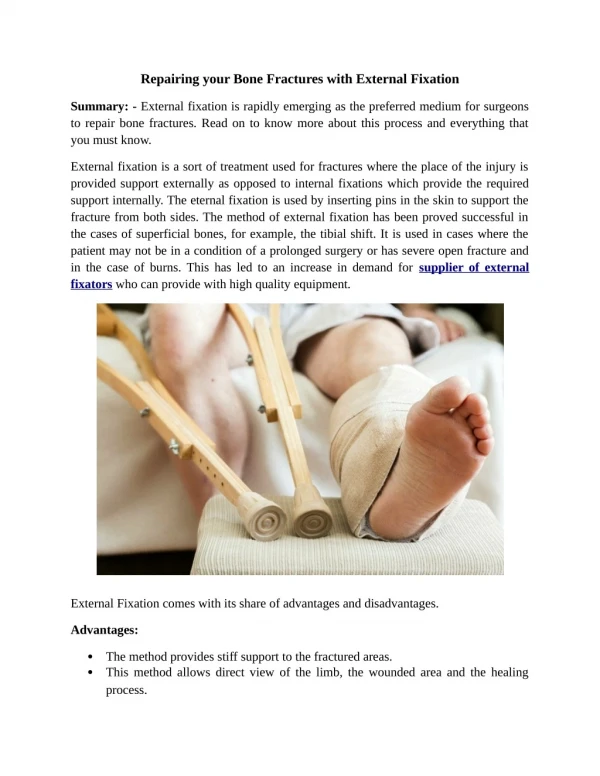
Treatment of the Acromioclavicular Joint Dislocation with External Fixation Device. Chelnokov A.N. Tyrtseva E.S. Ural Scientific Research Institute of Traumatology and Orthopaedics, Ekaterinburg, Russia. Background.

E N D
Treatment of the Acromioclavicular Joint Dislocation with External Fixation Device Chelnokov A.N. Tyrtseva E.S. Ural Scientific Research Institute of Traumatology and Orthopaedics, Ekaterinburg, Russia
Background • To date there has been no consensus about optimal treatment of the traumatic dislocation of the acromio-clavicular joint.
Many treatment modalities for the ACJ dislocation • From aggressive surgery…
…to nonoperative management • A Prospective Evaluation of Untreated Acute Grade III Acromioclavicular Separations. T.F. Schlegel. The American Journal of Sports Medicine 29:699-703 (2001): • 20 of the 25 patients completed the 1-year evaluation and strength-testing protocol; • objective examination and strength testing of the 20 patients revealed no limitation of shoulder motion in the injured extremity and no difference between sides in rotational shoulder muscle strength
Aim of this study was to estimate capabilities of small wire monolateral external fixator for closed treatment of complete acromioclavicular dislocations.
6 10 8 Material and methods • 24 patients • 14 male • 10 female • 3,2 days after the injury (0-14)
External Fixation • G.S.Sushko, G.A.Ilizarov, 1977, 1979
Surgery and post-op period • 10-30 minutes • Regional anesthesia • Discharge in 1-2 days • Sling for 1-3 days
Duration of fixation • 4 weeks for acute cases (fixation within 0-5 days after the injury), • 6-8 weeks for delayed admission (6-14 days) • In cases of dislocations older 2 weeks => AC and CC ligaments repair by tendon allografts • Stability test before hardware removal
Results • Self-care, light housework – 3-5 days • Deep infection 0/24 • 10 patients (42%) sustained skin irritation and serum drainage from acromial wire site only • 23/24 healed • 1/24: missed acromial wire cut-out => symptomatic instability => AC+CC repair (allo tendons) => uneventful healing • 1 year follow up - 15 patients. • All restored their pre-injury status • Occasional pain in hyperabduction – 3/15
Follow-up (3 years) Affected side
Discussion: Advantages of the technique • Controllable fixation • With ex-fix we control the situation, without it the situation controls us • Minimally invasive • Fast recovery • Good cosmetic effect • Minimal time and efforts • Short learning curve
Discussion: Disadvantages • Temporary discomfort, decreased quality of life • Pin site care, outpatient visits necessary • Hardware removal
Conclusion • External fixation can be technique of choice for acute cases where operative treatment is indicated
Thank you http://weborto.net