Download
1 / 134
1.36k likes | 1.42k Views
Orthopedic surgery part

E N D
Complication and management of the dislocation of shoulder joint, elbow joint and hip joint Submitted by- RATNESH KUMAR SHUKLA B. A. M. S. FINAL YEAR Submitted to – DR. VIKAS KHARE (M. S. , H. O. D.)
Component:- • Definition • Types of dislocation • Dislocation • Typical deformities in dislocation • Investigation • Treatment • Complication • Caution • Remember in dislocation
Definition • It is complete and persistent displacement of a joint . • This is a condition in which one bony component loses its contact completely with the other bony component of the joint. • If it retains partial contact, the term sub-luxation is applied.
Types of dislocation • Congenital • Acquired • Traumatic • Pathological e.g. Septic Arthritis • Paralytic e.g. Poliomyelitis, etc • Inflammatory disorders, rheumatoid arthritis,etc
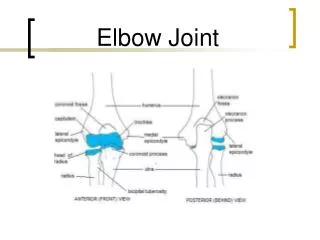
Dislocation • No joint is immune from dislocation • Most commonly occur in the following joints. • Shoulder • Hip • Elbow • Metacarpophalengealjoint • Facet joint dislocation in cervical spine. • Acromiclavicular joint dislocation.
Investigations • Radiograph of the affected part should include anterior posterior and lateral views and sometimes special views needed. • CT Scan • MRI
Treatment • Since dislocation is an orthopedic emergency, early closed reduction under general anesthesia is recommended. • The part is immobilized for a period of 3 to 6 weeks to ensure adequate healing. • Operative reduction is rarely required and is reserved for compound dislocations or irreducible dislocations.
Complication • Acute: Injury to peripheral nerve and vessels e.g. sciatic nerve palsy in posterior dislocation of hip • Chronic: • Unreduced dislocation - due to ignorance, delay in seeking treatment, etc. • Recurrent dislocation - Due to inadequate and improper healing of soft tissues following initial trauma, e.g. recurrent dislocation of the shoulder. • Traumatic osteoarthritis - Due to damage to the articular cartilage following impaired nutrition by the synovial fluid. • joint stiffness - Due to capsular and other soft tissue damage. • Avascular necrosis - Due to injury to the vessels. • Myositis osificans - More commonly seen than in fractures due to greater periosteal strip
Caution! • Excessive force should not be used in close reduction. • Forceful manipulation maylead to{fracture. • Interposition ofsofttissue, bonyfragment or buttonhole in capsule may make close reduction impossible.
RememberinDislocation • It is an orthopedic emergency. • Reduction should be quick and prompt. • Reduction should always be under G/A or sedation. • Swelling is less in compared to fractures. • Movements are more restricted than in fractures. • Closed reduction is sufficient in most of the times. • Open reduction is restored to if specifically indicated. • Reduction techniques should always be very gentle. i .Pain willnotsubside bysplinting unlike fractures.
Bhagna • The word Bhagna is derived from the “bhanj-dhatu” and “Katupratyaya” meaning to break. • In Ayurvedic literature no clear-cut definition of Bhagna is available. But onthe gmmmatical basis of terminolory, details of etiology and clinical features it can well beunderstood that the word pertains to the skeletal injury and can be defined as "'disruption in thecontinuity of the bone substance or incongruity of articulating bones is known as Bhagna' andincludes all the fractures, dislocations and subluxation . • CAUSATIVE FACTOR- a. Trauma is considered as the main cause of'Bhagna’. b. Mechanical causes e.g. Patana (falls), Peedana (compression), Prahara (blows), Alcshepana (Repeated and forceful muscular movements). Such injuries can occur in variety of situationslike domestic, industrial, roadside accidents or assaults eeetc.
Classification • Bhagna is an agantuja type of Vyadhi (disease) hence; there will be no specific pathology or pre-existing etiopathogenesis’. It has been classified in to two tlpes viz’ Sandhimoksha and Kandabhagna. • I. Sandhimukta (Joint injuries): This type of Bhagna includes sub-luxations' Dislocations’ Ligamentous and other soft tissue injuries arround the joint:
Aim of the local treatment is Kushabandhana (Splinting of • the injured part), Vednasthapana (To control pain), In case of associated Vrana (wound) or • Bleeding Raktastambhaka (To contRol bleeding), to protect against tetanus, gas gangrene and other • Infections, Vrana SAndhana (To promote wound healing).
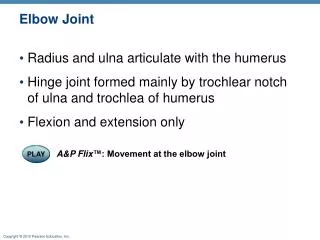
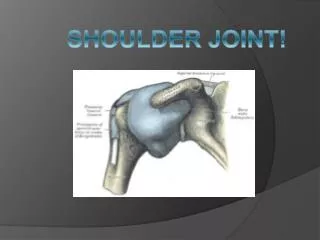
ANATOMY • The shoulder joint ( glenohumeral joint), is structurally classified as a synovialball and socket joint. • It involves articulation between the glenoid cavity of the scapula(shoulder blade) and the head of the humerus(upper armbone). • Due to the very loose joint capsule that gives a limited interface of the humerus and scapula, it is the most mobile joint of the human body. • However the socket of the glenoid cavity of the scapula is itself quite shallow and is made deeper by the addition of the glenoid labrum. • Like most synovial joints, the articulating surfaces are covered with hyaline cartilage.
Structures of the shoulder joint • Shoulder joint surrounded mainly By these structures:- • Joint capsule • Ligaments • Muscles • Bursae • Nerve and blood supply
Ligaments In the shoulder joint, the ligaments play a key role in stabilising the bony structures. • Glenohumeral ligaments (superior, middle and inferior) –
Ligament • Transverse humeral ligament – spans the distance between the two tubercles of the humerus. It holds the tendon of the long head of the biceps in the intertubercular groove.] • Coracohumeral ligament – attaches the base of the coracoid process to the greater tubercle of the humerus. It supports the superior part of the joint capsule. • coracoacromial ligament- between the acromion and coracoid process of the scapula it forms the coraco-acromial arch. This structure overlies the shoulder joint, preventing superior displacement of the humeral head.
Muscles • The Rotator Cuff Muscles These muscles are essential to the healthy functioning of the glenohumeral joint. They are a set of four muscles that run from the scapula to the humerus. As their tendons approach the humerus, they blend with the capsule, reinforcing it further. This group of muscles may also be referred to as the SITS muscles: • the supraspinatus, • infraspinatus, • teres minor, and • subscapularis.
Muscles • Accessory mucles Posterior muscle group • deltoid • latissimus dorsi • teres major
Muscles Anterior muscle group • pectoralis major • coracobrachialis • Biceps branchi
Nerve supply and blood supply • Axillary Nerve - supplies the Deltoid muscle. Most commonly stretched with shoulder dislocations. • Long Thoracic Nerve - supplies Serratus Anterior muscle and can cause Winging of the Shoulder • Suprascapular Nerve - supplies supraspinatus and infraspinatus muscles and can be entrapped or diseased.
Nerve and blood supply Blood supply • The shoulder joint is supplied with blood by branches of the anterior and posterior circumflex humeral arteries, the suprascapular artery and the scapular circumflex artery.
Mobility and stability Factors that contribute to mobility: • Type of joint – ball and socket joint. • Bony surfaces – shallow glenoid cavity and large humeral head – there is a 1:4 disproportion in surfaces. A commonly used analogy is the golf ball and tee. Factors that contribute to stability: • Rotator cuff muscles – surround the shoulder joint, attaching to the tuberosities of the humerus, whilst also fusing with the joint capsule. The resting tone of these muscles act to compress the humeral head into the glenoid cavity. • Glenoid labrum – a fibrocartilaginous ridge surrounding the glenoid cavity. It deepens the cavity and creates a seal with the head of humerus, reducing the risk of dislocation. • Ligaments – act to reinforce the joint capsule, and form the coraco-acromial arch. • Biceps tendon – it acts as a minor humeral head depressor, thereby contributing to stability.
Shoulder joint dislocation • Shoulder dislocations represent 50% of all major joint dislocations, with anterior dislocation being most common. • The shoulder joint is the most regularly dislocated joint in the body. The shoulder can dislocate forward, backward, or downward, and completely or partially, though most occur anteriorly. • Fibrous tissue that joins the bones can be stretched or torn, complicating a dislocation. • It takes a strong force, such as a blow to the shoulder to pull the bones out of place. Extreme rotation can pop the shoulder out of its socket. • contact sports injuries often cause a dislocated shoulder.
Causes Dislocation due to Anatomical causes:- • Shallow glenoid • ·Extraordinary Rotation Of Muscle • .Vulnerability of upper limb to injury • Underlying conditions eg. ligament laxity Dislocation due to traumatic causes :- • Sports injuries. Shoulder dislocation is a common injury in contact sports, such as football and hockey, and in sports that may involve falls, such as downhill skiing, gymnastics and volleyball. • Trauma not related to sports. A hard blow to your shoulder during a motor vehicle accident is a common source of dislocation. • Falls. You may dislocate your shoulder during a fall, such as from a ladder or from tripping on a loose rug.
Symptoms and sign • Significant pain, sometimes felt along the arm past the shoulder. • Sensation that the shoulder is slipping out of the joint during abduction and external rotation. • Numbness of the arm. • Visibly displaced shoulder. Some dislocations result in the shoulder appearing unusually square. • No palpable bone on the side of the shoulder.
Classification of shoulder joint dislocation Doctors classify shoulder dislocations into three types, depending on the direction of thedislocation: • Anterior Dislocations • Posterior dislocations • Inferior dislocations (luxatio erecta)
Anterior dislocation of shoulder joint • The top of the humerus is displaced forward, toward the front of the body. • This is the most common type of shoulder dislocation, accounting for more than 95% of cases. • In young people, the cause is typically sports-related. • In older people, it usually is caused by a fall on an outstretched arm.
Classification of anterior dislocation • Anterior dislocations can be further divided according to where the humeral head comes to lie: • subcoracoid: most common • subglenoid • subclavicular
Mechanism of anterior dislocation of shoulder joint • An anterior dislocation accounts for 97% of recurrent or first time dislocations. It is the most common dislocation and is caused by the arm being positioned in an excessive amount of abduction and external rotation. • In this position, the inferior glenohumeral complex serves as the primary restraint to anterior glenohumeral translation.[ • Due to a lack of dynamic stabilization, the glenohumeral joint is most susceptible to dislocation in the 90 degree abduction and 90 degree external rotation • Supporting structures that may be deficient in an anterior dislocation are the anterior capsule, long head of biceps, subscapularis, superior and middle glenohumeral ligaments. • When there is a thinning in the anterior capsule, it may present between the superior and middle glenohumeral ligaments. As a result of its inherent weakness, the humeral head is more prone to dislocate at this interval.
Clinical features • The patient complains of severe pain and inability to use the shoulder joint. • Flat shoulder, rounded anterior prominence and the arm held in a position of abduction and external rotation are some of the unmistakable clinical signs. • Due to injury to the axillary nerve, there could be loss of sensation on the outer aspect, of the upper arm and is called the ‘Regiment Badge’ sign ().
Radiographic examination • A set of shoulder X-rays is usually standard in diagnosing a shoulder dislocation. They are used to determine the presence of a dislocation, and also to check for other injuries . • In cases of severe injury CT scan also very useful.
Test for anterior dislocation of shoulder joint Dugas test Hamilton ruler test • Hamilton's ruler sign is positive when the tip of the acromion may be joined to the lateral epicondyle of the humerus with a straight line.
Management • Is an Emergency • It should be reduced in less than 24 hours or there may be Avascular Necrosis of head of humerus • Check AXILLARY NERVE FUNCTION Because the nerve is so vulnerable, it is important to test the function of the nerve record it before reduction is attempted. • Following reduction the shoulder should be immobilised strapped to the trunk for 3-4 weeks. • Anterior shoulder dislocations are usually managed with closed reductionand a period of immobilization (e.g. 6 weeks) to allow adequate capsular healing, although whether this significantly changes the likelihood of recurrent dislocation is not certain .
Methods of closed Reduction of anterior shoulder Dislocation • Hippocrates Method(anesthesia required) • Stimpson's technique (analgesia) • Kocher's technique is the method used in hospitals under general anesthesia and muscle relaxation. • Milch technique is the method in which the arm is abducted and externally rotated with thumb pressure applied to the humeral head.
Hippocratic method • The doctor holds the patients affected arm by wrist and applies traction at a 45 angle. At the same time provides counter traction by placing foot on the patients chest wall or having an assistant wrap a sheet around the patient.
External rotation method • The patient is kept in supine position on the bed. • The affected arm is adducted and flexed at 90 at the elbow. • The arm is then slowly -externally rotated. • The shoulder should be reduced before reaching the coronal l plane.
Stimson's technique • The patient is kept in prone position on bed. The affected shoulder is supported and the arm is left to hang over the edge of the bed.i • A weight is attached to the elbow or wrist. • It is usual to begin with 2kg up to 10 kg may be applied. Gravity stretches the muscles and reduction occurs.i • Gentle internal humeral rotation may be applied. This method takes 15 to 20 minutes.
KOCHER'S METHOD: - • The affected arm in bend at 90 at elbow, adducted against the body, the wrist and the point of the elbow is grasped by the doctor, slowly externally rotate between 70 to 85 until resistance is felt. • Lift the externally rotated arm in the sagital plane as far as possible forwards now internally rotate the shoulder this brings the patient hand towards the opposite Shoulder. • The humeral head is now slipped back into the glenoid fossa with pain eliminated during this process. • This method is not used frequently because of risk of fracture of humeral neck or shaft.
Milchtechnique • The arm is abducted and the physician's thumb isused to push the humeral head into its proper position. Gentle traction in line with the humerus is provided with the physician's opposite hand.
Care after closed reduction • Neurovascular assessment should be repeated • A post-reduction x-ray should be taken. • After reduction immobilized for 3-4 weeks. • Analgesics for pain • Physiotherapy should be done.
Surgical treatment of shoulder joint dislocation • Surgical repair is not required for dislocation per se, but rather to treat complications and associated injuries which include: • shoulder instability due to damage to the inferior glenohumeral ligament (IGHL) • Hill-Sachs lesion • Bankart lesion or other anterior glenolabral injuries • damage to the axillary artery, or brachial plexus • Recurrent shoulder joint dislocation
Surgical treatment of shoulder joint dislocation • Bankart repair is commonly used for people with anterior dislocations . Anterior dislocations can create a tear in the shoulder’s labrum, the cartilage around the shoulder’s socket. This kind of tear is known as a Bankart lesion. The torn labrum is repaired and re-anchored to the shoulder’s socket during a Bankart repair. • Latarjet procedure may be recommended for a person with bone loss at the shoulder’s socket. A Latarjet procedure involves taking a small amount of bone material from the coracoid process (part of the shoulder blade) and transferring it to the front part of the shoulder’s socket. Bone loss in the socket can also be repaired with bone grafts taken from the patient’s iliac crest (part of the pelvic bone) or from a donor. Bone grafts from a donor or bone bank may increase the risk of infection.
Surgical treatment of shoulder joint dislocation • Remplissage procedure • may also be needed if the shoulder’s ball, or humeral head, has been badly damaged by dislocation, causing a condition known as a Hill-Sachs lesion. The procedure involves resurfacing the head and/or filling in the defect by fixing it to part of the rotator cuff. • Capsular shift • tightens the ligaments surrounding the shoulder that have stretched and loosened because of multiple dislocations.
Recurrent anterior shoulder joint dislocation • This is a very common complication of anterior dislocation of shoulder and accounts for greater than 80% of dislocations of the upper extremity. • Age at the time of initial dislocation is an important prognostic factor, recurrence rate being 55% in patients 12 to 22 years old, 37% in 23 to 29 years old, and 12% in 30 to 40 years old.