Download

1 / 83
850 likes | 1.23k Views
Neurodegenerative D iseases. Neurodegenerative D iseases. These are diseases of gray matter characterized: by the progressive loss of neurons with associated secondary changes in white matter tracts. Neurodegenerative D iseases.

E N D
Neurodegenerative Diseases These are diseases of gray matter characterized: • by the progressive loss of neurons • with associated secondary changes in white matter tracts.
Neurodegenerative Diseases • The pattern of neuronal loss is selective, affecting one or more group of neurons. • A common theme is the presence of protein aggregates resistant to degredation through the ubiquitin-proteasome system.
Neurodegenerative diseases • Characterized by nerve cell loss and gliosis, often in specific regions of the brain which correlate with clinical symptoms • example: Huntington diseasecaudate nucleus • Specific or non-specific inclusions are common
Gross atrophy of the affected regions may be seen— • Examples: • Diffuse atrophy in Alzheimer disease, • Caudateatrophy in Huntington disease.
Neurodegenerative disorders • Degenerative diseases affecting the cerebral cortex • Alzheimer disease • Frontotemporal dementias • Pick disease • Progressive supranuclear palsy • Corticobasal degeneration • Vascular dementia • Degenerative diseases of basal ganglia and brain stem • Parkinson disease- Akinetic • Dementia with Lewy bodies • Huntington disease- Hyperkinetic • Spinocerebellardegenerations • Spinocerebellar ataxia • Friedrich ataxia • Ataxia telengiectasia • Degenerative diseases affecting motor neurons • ALS • Bulbospinal atrophy • Spinal muscular atrophy
Degenerative diseases affecting the cerebral cortex • Alzheimer disease • Dementia of frontotemporal lobe type ; DFLT) • Pick disease • Other • Vascular dementia (serebrosclerosis) • Dementia with hydrocephalus (NPH).
Dementia • Neuropathologically • Alzheimer disease 65% • Vascular disease 15-20% • Dementia with Lewy bodies 10% • Others: • Dementia of frontal lobe type • Pick disease (<2%)
Alzheimer's Disease • Degenerative; • The major cause of dementia in the elderly; • Main pathologic change is generalized atrophy of brain with neurofibrillary tangles, senile plaques and amyloid angiopathy in many parts of the brain.
Impairment of recent memory • Aphasia (naming), apraxia (motor), agnosia (object), executive functioning • Progressive over time • 47% of people over 85 years of age are affected • Familial cases with a defined inheritance pattern account for only 5 to 10% of Alzheimer's disease. • Familial cases tend to have an earlier age at onset. • Genetic defects in familial cases have been identified on chromosomes 21, 19, 14, 12 and 1.
Regardless of the cause, the diagnosis of AD is made clinically by the finding of progressive memory loss with increasing inability to participate in activities of daily living. • Late in the course of the disease, affected persons are not able to recognize family members and may not know who they are. • The definitive diagnosis is made pathologically by examination of the brain at autopsy. • Grossly, there is cerebral atrophy, mainly in frontal, temporal, and parietal regions. • As a consequence, there is ex vacuo ventricular dilation.
Alzheimer's disease leads to cerebral atrophy. The external surface of the brain with widened sulci and narrowed gyri, mostly over the frontal and parietal regions, gross.
Alzheimer's disease : the characteristic hydrocephalus ex vacuo, or ventricular dilation resulting from loss of cortex.
In the neuropil of the cerebral cortex there is fragmentation of neurites (neuronal processes) within gray matter producing the characteristic "senile plaques“. These are degenerative presynaptic endings. The plaques may also contain a few astrocytes, and microglia. Bielschowsky silver stain.
The thioflavin stain viewed with fluorescence microscopy highlights the neuritic plaques of Alzheimer's disease with amyloid deposition which fluoresces bright green, as shown here.
neurofibrillary tangle Older plaques contain a central amyloid core, seen here with Congo red stain. A small vessel demonstrates amyloid angiopathy as well.
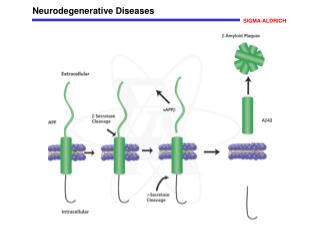
The pathologic changes of Alzheimer disease occur in nearly all Down syndrome (trisomy 21) patients by the age of 45. • Amyloid precursor protein (APP) • Abnormal APP processing leads to deposits of insoluble β-pleated amyloid protein resulting in fibrillar aggregates of beta-amyloid that is toxic to neurons.
Normal aging • Diffuse plaques and neuritic plaques: uncommon (20% of those studied) in 6th decade, common (90%) in centenarians • Neurofibrillary degeneration: uncommon in cortex in normal aging.
Alzheimer disease: Summary • Most common cause of dementia in the elderly • Degenerative cell loss leadsto gross atrophy of the entire brain with “hydrocephalus ex vacuo” • Neuritic plaques, neurofibrillary tangles, cell loss and gliosis, granulovacuolar degeneration, amyloid angiopathy, Hirano bodies.
Pick disease • Onset 45-65 years, rare after 75 • 80% are sporadic/20% familial • 5-10 year duration • Frontal lobe symptoms(personality changes, ‘haphazard’ behavior, lack of planning, antisocial, obsessive compulsive, language deficits, anomia and echolalia), • Anterior temporal lobesymptoms(aphasia, semantic memory loss, Kluver-Bucy syndrome) and pathology • memory relatively retained.
Gross appearance: severe localized atrophy of frontal lobes and anterior temporal lobes “knife-edge” atrophy • Microscopic appearance: Pick cells (ballooned neurons) and Pick bodies with cell loss and gliosis • Pick cells are seen in 1/2 of cases with typical gross appearance and Pick bodies only 20%
Pick's disease with the gross appearance of lobar atrophy is seen here involving the frontal lobe. Note the "knife like" gyri.
Pick's disease is demonstrated grossly in this coronal section in which there is marked atrophy with ex vacuo ventricular dilation.
Multi-infarct dementia (MID) • Multi-infarct dementia (MID) can cause a dementia similar to Alzheimer's disease (AD). • However, no pathologic findings are present characteristic of AD. • Instead, there are multiple ischemic lesions in the cerebral cortex that cumulatively result in loss of enough neurons to produce dementia.
Most patients with MID have an abrupt onset of cognitive symptoms along with an incremental loss of mental function. • Focal neurologic deficits can be present, depending upon the size and location of the infarcts. • In some cases, though, there is gradual loss of mental function.
Pathologically, • marked cerebral arterial atherosclerosis and/or • thromboembolic disease can account for the appearance of many infarcts, typically small and scattered.
Grossly, this composite view of the brain demonstrates multiple remote cystic infarcts in various locations. This process took several years.
Movement disorders • Akinetic-rigid • Parkinson disease (PD) Postencephalitic parkinsonism (PEP) • Multiple system atrophy (MSA)
Parkinson disease • Idiopathic Parkinson disease (vs. parkinsonism or parkinsonian syndrome) • Tremor (rest) • Rigidity (cogwheel rigidity) • Bradykinesia (mask-like facies, loss of arm-swing) • Festinating gait (loss of righting reflexes)
Gross: loss of pigment in the substantia nigra • Microscopic : Lewy bodies with pigmented neuronal cell loss and gliosis • cortical Lewy bodies present in 80% or more of PD cases
Most cases are sporadic. • Mechanism: Loss of dopaminergic input from substantia nigra to striatum • This syndrome covers several diseases of different etiologies which affect primarily the pigmented neuronal groups including the • substantia nigra, • locus ceruleus, • dorsal motor nucleus of cranial nerve X, • the substantia innominata.
The pigmented neurons are slowly lost as the disease progresses and melanin pigment can be seen within the background neuropil or within macrophages. • Astrocytosis occurs secondary to neuronal loss. • Some patients with Parkinsonian symptoms also have dementia, and in these patients there are Lewy bodies in the cerebral cortex, as well as the substantia nigra.
Pathology • Lewy bodies in association with Parkinson's disease are found within the cytoplasm of pigmented neurons. • For a diagnosis of DLB, the Lewy bodies must be found in the neocortex. • These are homogeneous pink bodies on H&E stains with a surrounding halo. • Immunohistochemical staining with antibody to alpha-synuclein is positive in these Lewy bodies.
A normally pigmented substantia nigra The patient with Parkinson's disease has decreased neurons and pigment as seen microscopically at the right
Other parkinsonian syndromes • Differential diagnosis of parkinsonism • Progressive supranuclear palsy (PSP) • Corticobasal degeneration (CBD) • Multiple system atrophy (MSA) • striatonigral degeneration • olivopontocerebellar atrophy • Shy-Drager syndrome • Dementia pugilistica • Postencephalitic parkinsonism (PEP)
Parkinson disease summary • Akinetic movement disorder • Loss of dopaminergic input from substantia nigra to striatum • Pigmented (neuromelanin containing) nerve cell loss with gliosis in the substantia nigra pars compacta and locus ceruleus (pigment loss is grossly apparent) • Lewy body formation in brainstem and cortex.
Parkinson disease and dementia • Relatively common disorder in the middle-aged and elderly; • The major pathologic changes are seen in the pigmented neurons of the substantia nigra in the midbrain; • neurons in this area contain intracytoplasmic inclusions called Lewy bodies.
40% of Parkinson Disease patients develop dementia; • demented PD patients have more Alzheimer disease pathology than non-demented PD patients • some demented PD patients have only Lewy body pathology
Dementia with Lewy Body Diseases (DLB) Dementia with Lewy bodies is a clinicopathological syndrome that may account for up to 20% of all cases of dementia in older patients, typically in their seventh and eighth decades.
DLB There are three major syndromes associated with the appearance of Lewy bodies. These are: • (1) Parkinson disease, • (2) autonomic nervous system failure, • (3) dementia.
The clinical presentation of Lewy body disease varies according to the site of Lewy body formation and associated neuronal loss. • In Parkinson disease, the Lewy bodies are found in the substantia nigra of the midbrain, coupled with the loss of pigmented neurons. • In persons with the dementia of diffuse Lewy body disease, there are Lewy bodies in the neocortex. • Some persons have the Lewy bodies in both locations. • The basal ganglia and diencephalon may also be involved in some cases.
H&E stain demonstrates a rounded pinkcytoplasmic Lewy body in a neuron of the cerebral cortex from a patient with diffuse Lewy body disease, which can be a cause for dementia. Lewy bodies can also be seen in substantia nigra with Parkinson's disease. An immunoperoxidase stain for ubiquitin, seen at the right, helps demonstrate the Lewy bodies more readily by the brown reaction product within them. Lewy bodies • spherical, intraneuronal, cytoplasmic, eosinophilic inclusions.
Multiple system atrophy (MSA) • Prevalence: 8% of parkinsonian cases in PD brain banks • Microscopic finding: oligodendroglial cytoplasmic inclusions • Clinical signs and symptoms • Parkinsonism (striatonigral degeneration) • Autonomic failure (Shy-Drager syndrome) • Cerebellar findings (olivopontocerebellar degeneration)
Striatonigral degeneration • parkinsonism with orthostatic hypotension and cerebellar ataxia • cell loss and gliosis in putamen • Olivopontocerebellar atrophy (sporadic) • neuronal loss and gliosis • Shy-Drager syndromesympathetic ganglia
Movement disorders • AkineticPD, other diseases with parkinsonian features • Hyperkinetic • Huntington chorea • Other • Myoclonus • Ballismus • Dystonia • Tic disorders
Huntington’s disease • Choreiform movements, neuropsychiatric disturbance and slowly progressive dementia • seizures or rigidity may occur initially • Gross:atrophic, flattened caudate • Microscopic:cell loss and gliosis in caudate nucleus (dorsal putamen, globus pallidus and nucleus accumbens affected later)
Huntington's disease is shown grossly in this coronal section of the brain. It demonstrates atrophy of the caudate with resultant increase in size of lateral ventricles.