Download
1 / 1
10 likes | 75 Views
Discover the substantial decline in pertussis cases in Massachusetts post introduction of Tdap vaccine in 2005. Our research shows a direct correlation between adolescent Tdap vaccination and decreased pertussis rates in infants.

E N D
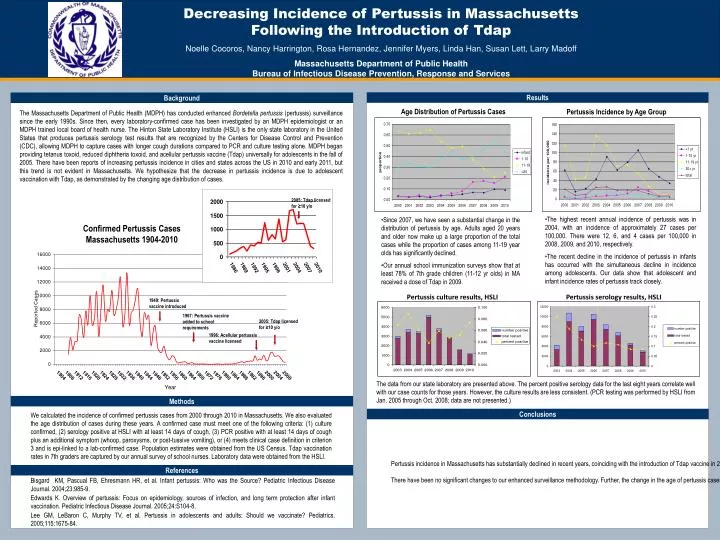
Results Background The Massachusetts Department of Public Health (MDPH) has conducted enhanced Bordetella pertussis (pertussis) surveillance since the early 1990s. Since then, every laboratory-confirmed case has been investigated by an MDPH epidemiologist or an MDPH trained local board of health nurse. The Hinton State Laboratory Institute (HSLI) is the only state laboratory in the United States that produces pertussis serology test results that are recognized by the Centers for Disease Control and Prevention (CDC), allowing MDPH to capture cases with longer cough durations compared to PCR and culture testing alone. MDPH began providing tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine (Tdap) universally for adolescents in the fall of 2005. There have been reports of increasing pertussis incidence in cities and states across the US in 2010 and early 2011, but this trend is not evident in Massachusetts. We hypothesize that the decrease in pertussis incidence is due to adolescent vaccination with Tdap, as demonstrated by the changing age distribution of cases. Age Distribution of Pertussis Cases Pertussis Incidence by Age Group 2005: Tdap licensed for ≥10 y/o • The highest recent annual incidence of pertussis was in 2004, with an incidence of approximately 27 cases per 100,000. There were 12, 6, and 4 cases per 100,000 in 2008, 2009, and 2010, respectively. • The recent decline in the incidence of pertussis in infants has occurred with the simultaneous decline in incidence among adolescents. Our data show that adolescent and infant incidence rates of pertussis track closely. • Since 2007, we have seen a substantial change in the distribution of pertussis by age. Adults aged 20 years and older now make up a large proportion of the total cases while the proportion of cases among 11-19 year olds has significantly declined. • Our annual school immunization surveys show that at least 78% of 7th grade children (11-12 yr olds) in MA received a dose of Tdap in 2009. Confirmed Pertussis Cases Massachusetts 1904-2010 Pertussis culture results, HSLI Pertussis serology results, HSLI 1949: Pertussis vaccine introduced 1967: Pertussis vaccine added to school requirements 2005: Tdap licensed for ≥10 y/o 1996: Acellular pertussis vaccine licensed The data from our state laboratory are presented above. The percent positive serology data for the last eight years correlate well with our case counts for those years. However, the culture results are less consistent. (PCR testing was performed by HSLI from Jan. 2005 through Oct. 2008; data are not presented.) Methods We calculated the incidence of confirmed pertussis cases from 2000 through 2010 in Massachusetts. We also evaluated the age distribution of cases during these years. A confirmed case must meet one of the following criteria: (1) culture confirmed, (2) serology positive at HSLI with at least 14 days of cough, (3) PCR positive with at least 14 days of cough plus an additional symptom (whoop, paroxysms, or post-tussive vomiting), or (4) meets clinical case definition in criterion 3 and is epi-linked to a lab-confirmed case. Population estimates were obtained from the US Census. Tdap vaccination rates in 7th graders are captured by our annual survey of school nurses. Laboratory data were obtained from the HSLI. Conclusions Pertussis incidence in Massachusetts has substantially declined in recent years, coinciding with the introduction of Tdap vaccine in 2005. MDPH now provides Tdap for all children aged 7 through 18 years of age in our state; our 2009 annual school immunization survey shows that at least 78% of 7th grade children received a dose of Tdap. Adolescents have been identified as a major source of infection to infants (Bisgard et al., 2004; Edwards, 2005). Studies have predicted that vaccination of adolescents would result in a decline in infant pertussis cases (Lee et al., 2005). Our data suggest that the decrease in infant incidence rates is likely due to the decline in adolescent incidence. There have been no significant changes to our enhanced surveillance methodology. Further, the change in the age of pertussis cases in Massachusetts in recent years is consistent, and our serologic laboratory data track with incidence in recent years. Therefore, we conclude that the steady decline in pertussis incidence in Massachusetts is likely due to the use of Tdap among adolescents. We believe that the ability to universally supply Tdap for adolescents, regardless of insurance status, is key to adequate vaccine coverage and ultimately, pertussis control. References Bisgard KM, Pascual FB, Ehresmann HR, et al. Infant pertussis: Who was the Source? Pediatric Infectious Disease Journal. 2004;23:985-9. Edwards K. Overview of pertussis: Focus on epidemiology, sources of infection, and long term protection after infant vaccination. Pediatric Infectious Disease Journal. 2005;24:S104-8. Lee GM, LeBaron C, Murphy TV, et al. Pertussis in adolescents and adults: Should we vaccinate? Pediatrics. 2005;115:1675-84.






















