Download
1 / 17
170 likes | 347 Views
Chapter 17: IR to Infectious Disease. In BIOL 304, we examined how pathogens can establish an infection in a susceptible host Re: the 7 components of pathogenicity !! On the other hand, humans are defended by: Physical barriers of epithelia and skin Surface chemicals, enzymes, acids

E N D
Chapter 17: IR to Infectious Disease • In BIOL 304, we examined how pathogens can establish an infection in a susceptible host • Re: the 7 components of pathogenicity!! • On the other hand, humans are defended by: • Physical barriers of epithelia and skin • Surface chemicals, enzymes, acids • Competitive flora • Complement and sIg • Phagocytic cells • Specific/Adaptive IR
Still, infectious disease kills millions each year *Mostly, from bacterial and viral diseases
Anti-viral protection: Innate • Type I IFN’s (α & β) are triggered from infected cells • IFN’s bind to nearby cells and activate JAK-STAT pathway • Induces several gene products which function to: • Degrade viral RNA • Shuts down PS in infected cells
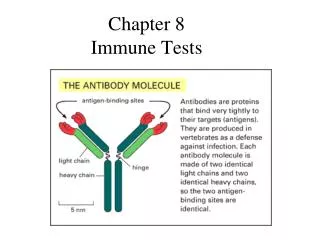
Anti-viral protection: Adaptive Neutralization by Ab’s • If Ig can bind to viral surface, prevents binding to target cell • Or Ig can trigger Complement cascade • Or bound Ig can agglutinate viruses to be phagocytized • sIgA blocks binding to mucosal surfaces
Anti-viral protection: Adaptive • Cell-mediated response • Starts with TH1 cells • Release of cytokines: • IL-2, IFN-γ, TNF • IL-2/IFN- γ act. NK cells • IL-2 recruits TC cells • Within 7-10 days, most virions are elim; parallels the development of Tc’s vs the virus
Evasion of Host defenses • Block intracellular effects of IFN’s (Hep C) • Block TAP function for Ag delivery to MHC I (HSV1 and 2) prevents lysis by Tc’s • Block formation of MHC I (Adenovirus, CMV) • Block formation of MHC II (CMV, measles, HIV) • Block complement fixation (Vaccinia binds to C4b*; HSV binds to C3b**) • Antigenic variation (influenza, rhinovirus, HIV) • Imunosuppression thru immune cell infection
Case study in viral mutation: Influenza • HA binds to host cells • NA aids in viral escape from host cells • 8 RNA’s code for 10 proteins • 3 types (A,B, and C) • Type A resp. for pandemics • 13 dif’t HA’s; 9 dif’t NA’s • WHO nomenclature of Type A: Ex: A/Sw/Iowa/15/30 (H1N1)
Case study in viral mutation: Influenza • Antigenic change is so complete no herd immunity can build • Ag variation occurs in HA and NA from: Antigenic Drift Antigenic Shift 1934 – H0N1 1947 – H1N1 1957 – H2N2 1968 – H3N2 1977 – H1N1 1989 – H3N2 *Each Ag shift results in new pandemic outbreaks **current vaccine has both H3N2 & H1N1 strains
Anti-bacterial protection • Bacterial infections are controlled by different IR’s (just as in viral infections) • The type of IR centers on: • Amount of inoculum • Degree of virulence • Extra- vs intra-cellular infection • MO’s enter mostly through mucosal surfaces (resp/g.i tract/g.u. tract) • Cuts/breaks in skin
IR’s to Extra-cellular infections • Stim production of humoral Ab’s from local lymph nodes. Ab’s function to: • Opsonize bacteria phagocytosis • Opsonize toxins inactivation • Bind/activate complement cell lysis • Stimulate/amplify inflammation mast cell degran • Chemotaxis
IR’s to Intra-cellular infections • Induce a Delayed-type hypersensitivity rxn • Cytokines, notably IFN-γ from CD-4 T cells activate MØ Cell-Mediated response
Evasion of Host Defenses • Major steps to bacterial infection: • Attachment • Proliferation/growth • Invasion • Toxin-induced damage • Host defenses operate during each one of these steps
Examples of pathogen control Diptheria • Classic example of imm bestowed by toxoid • 1923-Ramon inactivated exotoxin w/ formaledhyde • Significant drop in # of cases since then • Toxoid administered in DTP immuniz @6-8 wks w/ boosters every 10 yrs
Examples of pathogen control Tuberculosis • Inhaled bacilli ingested by alveolar MØ • Bacilli grow in and lyse MØ • Cytokines (esp IFN-y) produced by TH1 cells activates MØ to kill/ inhibit bacteria • MØ wall off bacilli at focal points in the lungs – in tubercles (granulomas) • MØ secrete IL-12 -> continue TH1 response • 10% progress to chronic pulmonary or extra-pulmonary TB
Emerging Infectious Diseases • Newly described pathogens • Those (which were once under control) showing rapid increases = “re-emerging infectious disease” Ex: TB Diptheria • Causes of emerging/re-emerging diseases: • Overcrowding in cities among lower socioeconomic populations • International travel • Mass distribution of food commodity