Download
1 / 20
210 likes | 1.01k Views
TYPES OF ANAEMIA. haemorrhagic. regenerative. haemolytic. Anaemia. primary B-M disorders . non regenerative. secondary B-M disorders. H A EMOLYTIC A NAEMIA. Total plasma protein within reference range or Plasma can be icteric or haemolysed.

E N D
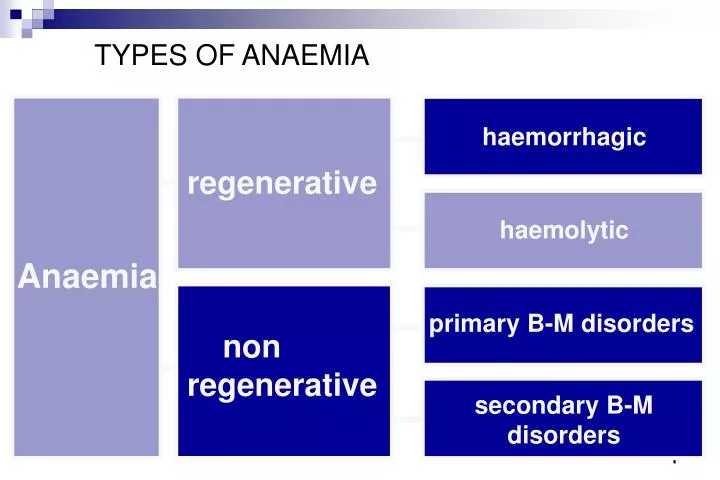
TYPES OF ANAEMIA haemorrhagic regenerative haemolytic Anaemia primary B-M disorders non regenerative secondary B-M disorders
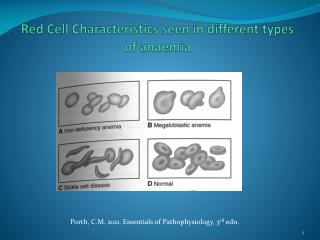
HAEMOLYTICANAEMIA Total plasma protein within reference range or Plasma can be icteric or haemolysed Abnormal erythrocyte morphology (spherocytes, Heinz bodies, RBC parasites) may suggest a haemolytic cause for the anaemia In haemolytic anaemia the plasma frequently appears yellow (icteric) due to increased RBC destruction and increased bilirubin metabolism. In severe haemolysis, haemoglobinaemia (producing red colour in plasma) and haemoglobinuria (producing red colour in urine) may result from the inability of the monocyte macrophage system to metabolise the large amounts of Hb being released.
IN REGENERATIVE ANAEMIAS: TPP and plasma colour can be used to differentiate haemolysis and haemorrhage Haemolytic anaemia Haemorrhagic anaemia TPP > 60 g/L PLASMA ICTERIC/ HEMOLYSED TPP < 60 g/L PLASMA CLEAR
HAEMOLYTICANAEMIA Clinical signs associated with an increase in haemoglobin catabolism: • Haemoglobinemia and haemoglobinuria • Icterus Icteric tissues when serum bilirubin levels >50mol/L Icteric serum when serum bilirubin levels >20mol/L
HAEMOLYTICANAEMIA Red blood cell lysis may occur by two mechanisms: 1.INTRAVASCULAR HAEMOLYSIS 2. EXTRAVASCULAR HAEMOLYSIS
INTRAVASCULAR HAEMOLYSIS (causes) • - Parasites/infectious causes • Babesia, Mycoplasma haemofelis, toxins (Leptospira, Clostridium). • Vascular Endothelial Lesions • haemangiosarcomas, DIC?, splenic torsion, heartworm disease. • Oxidant damage • onions, snake venom, methylene blue, acetaminophen. • Others • poisoning with Cu and Zn, genetic(pyruvatekinase/phosphofructokinase deficiency), severe hypophosphataemia.
INTRAVASCULAR HAEMOLYSIS (laboratory findings) In addition to PCV, TPP within the reference range or and icteric/haemolysed plasma • -Parasites/infectious causes: Blood smears, Serology/PCR • Vascular Endothelial Lesions: Schistocytes in blood smears • - Oxidative damage: Heinz bodies in blood smears
Heinz bodies Schistocyte
EXTRAVASCULAR HAEMOLYSIS -Physiological. (aged erythrocytes)removed by the macrophage-monocyte system in the spleen -Pathological. Auto-antibodies are produced against “normal” erythrocytes that are phagocytosed by the spleen - INMUNE-MEDIATED HAEMOLYTIC ANAEMIA
IMMUNE-MEDIATED HAEMOLYTIC ANAEMIA - Idiopathic (unknown mechanisms) - Secondary to: •Infectious agents •Drugs/insecticides/vaccines/neonatal isoerythrolysis CAUSE THE APPEARANCE OF ABNORMAL ANTIGENS ON THE ERYTHROCYTE CELL MEMBRANE
IMMUNE-MEDIATED HAEMOLYTIC ANAEMIA (laboratory findings) In addition to PCV, TPP= within the reference range or and yellow coloured plasma Spherocytosis Autoagglutination
Immune-mediated haemolytic anaemia • Categorised into two groups • Isoantibodies which pre-exist naturally or after exposure to isoantigens • Autoantibodies induced to self-antigens
Isoerythrolysishaemolytic disease of the new born • Maternal isoimmune blood group antibodies access and destroy foetal or neonatal RBCs • Isoantigens are antigens which can induce antibody formation in a member of the same species
Isoerythrolysis • Dam may be sensitised to foreign blood group • During pregnancy • At parturition • After vaccination (vaccines containing blood products) • After injection of blood or blood products
Isoerythrolysis • In the foetal/neonate circulation antibodies react with isoantigens on RBCs • RBCs are destroyed by phagocytosis or intravascular lysis
Haemolytic disease of the newborn Dam At parturition Vaccines Blood(products) Sensitisation to foreign Ag Formation of isoantobodies Foetus/neonate Entry to foetal or neonate circulation Destruction of red cells Phagocytosis Intravascular lysis
TESTS TO CHARACTERIZE • IMMUNE-MEDIATED HAEMOLYTIC ANAEMIA • COOMBS TEST • - ERYTHROCYTE FRAGILITY TEST
C3b IgG Poly specific serum agglutination THE COOMBS TEST The assay, using antisera against IgG, IgM and C3 (complement), detects the presence of these factors on RBC surface. Washed RBCs from the patient are mixed with antisera and a positive reaction is denoted by marked clumping of RBC.
COOMBS TEST Detects antibodies directed at the erythrocyte membrane False +ve: - some chronic infections - “ parasites (heartworms, haemobartonella) - “ drugs (trimethoprim-sulfa) - “ neoplasms False -ve: in some cases of inadequate antibody production The test is species-specific
ERYTHROCYTE FRAGILITY TEST: BASIS Whole blood in a hypotonic solution (0.55% NaCl) Normal RBCsabsorb water from the hypotonic solution for osmotic equilibrium and are distended but not haemolyzed Membranes of fragile RBCs (spherocytes cannot withstand distension and are bursted) Spherocytes are small and dense, and do not have central pallor, so can be easily detected in canine blood smears since normal erythrocytes have central pallor. The erythrocyte fragility test can be a help for detecting spherocytes in species with erythrocytes without central pallor.