Download
1 / 17
170 likes | 283 Views
Applying SNOMED CT codes for Electronic Health Records in the Netherlands. William Goossen RN PhD Senior researcher. Copenhagen, October 2006. Content of the presentation. Introduction and background Description of the study Results Conclusion. Introduction.

E N D
Applying SNOMED CT codes for Electronic Health Records in the Netherlands William Goossen RN PhD Senior researcher Copenhagen, October 2006
Content of the presentation • Introduction and background • Description of the study • Results • Conclusion
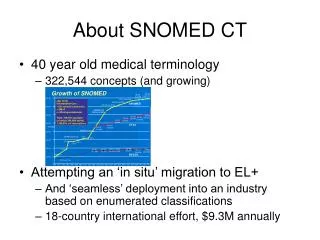
Introduction • NICTIZ, the Dutch National IT Institute for Health care, promotes standardization in the domain of care. • For the EHR development for the domain of stroke a template was developed: care information model. • For these models unique codes were needed, SNOMED CT was explored to see if it could provide unique codes.
SNOMED CT • SNOMED Clinical Terms (SNOMED CT) is a dynamic, scientifically validated clinical health care terminology and infrastructure. • SNOMED CT can be used for electronic medical records, ICU monitoring, clinical decision support, medical research studies, clinical trials, computerized physician order entry, disease surveillance, image indexing and consumer health information services.
Background • Development of an EHR for the complete chain of care for stroke patients • Standardization method: Health Level Seven version 3 (HL7 v3) • 84 ‘templates’ describing scales, instruments, observations and actions: care information models • An additional coding system is needed! • Temporary solution: invent new codes
Types of standards for healthcare • Clinical care standards: evidence based practice and guidelines: focus is quality of care • Terminology: focus is quality of documentation and understanding of meaning • Information models: focus is (electronic) exchange of information (semantic interoperability) • Workflow standards: focus is improvement and support of process of care • Technical standards: focus is quality of technology • In projects we try to combine these all for development of messages and EHRs.
Care information model • Care information models can be (validated) scales or instruments, observations or actions. • They represent best practice, are Health Level 7 compliant, support the uptake of standardized terminologies and facilitate technical implementation in both message and clinical information systems.
A care information model consists of 12 paragraphs: 1: version management 2: the aim of the instrument, observation or action. 3: the (scientific) foundation or evidence base. 4: the variables and their values. 5: the instructions for use of the instrument or observation. 6: interpretation guidelines. 7: references. 8: an example of the instrument 9: a description of the HL7 model and the model itself. 10: the mapping table from the domain to the HL7 Domain Information Model. 11: an XML message fragment. 12: remarks. It is open source, some are in English available, translation upon request. www.zorginformatiemodel.nl Content care information model
Description of the study Research questions: • For how many of the codes of the clinical concepts in the care information models can we find unique SNOMED CT codes? • Is there a difference for individual concepts and concepts representing scientific scales or measurement instruments with clinimetric characteristics?
Description of the study (2) Search strategy: • Translate the Dutch concepts into English • Start searching with the translated concept • No perfect match search for a concept on the SNOMED CT hierarchical levels above • No perfect concept search with synonyms • Still no perfect match search using the SNOMED CT hierarchy from top down
Description of the study (3) • The search for items was described in documents, together with the results • Then the results were examined by an expert on medical terminology • After that the SNOMED CT codes were added to the mapping table in the care information models
Results: quantitative Agreement on 89% of the concepts between coder and expert. For the self made codes 43% could be found in SNOMED CT. And for the codes from an existing coding system 70%.
Results: qualitative • A compound concept does not always relate to one SNOMED CT concept • Terminology of the clinical area could not always be found in SNOMED CT • Translation of some Dutch items could not be found • Items with left and right indications were hard to find • Level of detail differs • Cultural differences (use of stimulants is seen as abuse)
Discussion • The items for the care of stroke patients need a large granularity (very fine grained details) • Scales have specific clinimetric characteristics, that require an accurate equivalence between the items as used in practice and in the clinical terminology used for the unique coding • Translations errors and/or cultural differences might be of importance
Conclusions SNOMED CT is a useful coding system because: • Sufficient codes could be found, thus improving interoperability • It is possible to request for inclusion and coding of concepts that could not be found • SNOMED CT has an ongoing project for scale representation that takes the clinimetric aspects of scales and concepts into account • SNOMED CT is working on further internationalization in order to meet European requirements
What’s next? • Netherlands considers seriously to participate in International SDO Snomed CT • Continue ongoing use in NL (decades) • Use as reference terminology for international message exchange • Step by step introduction in the field • E.g. starting with diabetes project, perhaps introducing in current projects where it would not delay ongoing implementation work: care information model by care information model
dr William Goossen On behalf of NICTIZ, the national ICT institute for health care in the Netherlands www.nictiz.nl Researcher and consultant Acquest Dorpsstraat 50 2396 HC Koudekerk aan den Rijn + 31 71 541 9594 acquest@acquest.nl www.acquest.nl