Download
1 / 44
440 likes | 760 Views
Innervation of face . The main clinical syndromes of some Cranial Nerves’ ( Trigeminal , Facial , Glossopharyngeal) lesion. Trigeminal nerve nuclei. Nucleus of Pons Nucleus of spinal cord pathway Nucleus of midbrain pathway Motor nucleus. Trigeminal nerve functions.

E N D
Innervation of face. The main clinical syndromes of some Cranial Nerves’ (Trigeminal, Facial, Glossopharyngeal) lesion
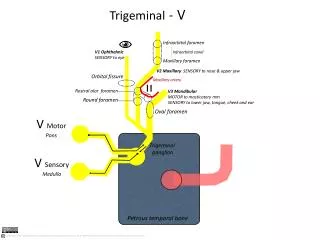
Trigeminal nerve nuclei • Nucleus of Pons • Nucleus of spinal cord pathway • Nucleus of midbrain pathway • Motor nucleus
Trigeminal nerve functions • Motor (innervation of masseter muscles) • Sensory • Autonomic
Symptoms of Trigeminal nerve’s lesion • facial pain • sensory disturbance in face • corneal reflex is decreased or absent • temporal and masseter muscles are atrophic or hypotrophic, atonic or hypotonic • jaw is deviated to the side of lesion
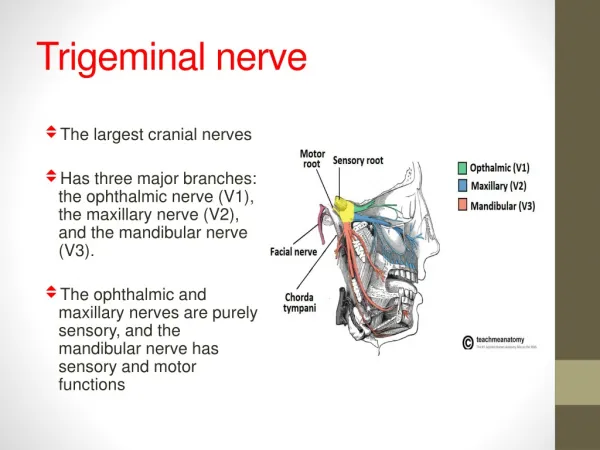
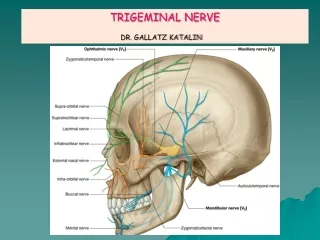
Trigeminal nerve branches • Ophthalmic nerve • Maxillary nerve • Mandibular nerve
Ophthalmic nerve • Lacrimal branch(innervation of lacrimal gland, upper eyelid, external corner of eye) • Frontal branch(n. Supraorbitalis – innervation of frontal skin, n. Supratrochlearis – upper eyelid, medial corner of eye) • Nasociliary branch(innervation of eyeball, mucous membrane of labyrinth, frontal sinus)
Maxillary nerve • Meningeal branch • Sphenopalatine nerve (for sphenopalatine ganglion) – major and minor palatine nerves, inferior posteriornasal nerves – mucous membrane of nasal cavity, palatal mucous membrane • Cheek bone nerve (anterior part of temporal and posterior part of frontal area, secretion parasympathetic fibers of lacrimal gland) • Nerve Infraorbitalis – upper alveolar nerves (posterior, medial, anterior), inferior branches of eyelids, external and internal nasal branches,upper branches of lips)
Mandibular nerve • Meningeal branches • Masticator nerve • Deep temporal branches • External sphenopalatine nerve • Internal sphenopalatine nerve • Buccal nerve • Temporal-ear nerve • Lingual nerve • Inferior alveolar nerve • Communicants branches for ear, hypoglossal and submandibular ganglions
Innervation of teeth • N. Infraorbitalisupper alveolar nerves (posterior, medial, anterior) upper dentalplexus(teeth, gums, paradontal, periodontal, mucous membrane of alveolar processes) • Mandibular nerveinferior alveolar nervesinferior dental plexus (at ½ of person)
Trigeminal nerve Clinical examination • testing pain, thermal, and other sensations in the area supplied by the Trigeminal nerve • the corneal reflex test • the temporal and masseter muscles are examined by palpating the muscles and attempts to resist the jaw by applying pressure
Pain, numbness in innervating zone Mononeuritic type of sensory disorders of all kinds of sensation Painful palpation of upper trigeminal point Decreased or absent subeyebrow, corneal and conjunctival reflexes Signs of lesion of the І branches of Trigeminal nerve
Pain and numbness in innervating zone Mononeuritic type of sensory disorders of all kinds of sensation Painful palpation of medial trigeminal point Signs of lesion of the ІIbranches of Trigeminal nerve
Pain, numbness in innervating zone Mononeuritic type of sensory disorders of all kinds of sensation Painful palpation of lower trigeminal point Decreased or absent the mandibular reflexes Disorders of jawing, atrophy or hypotrophy of masseter muscles Signs of lesion of the ІIIbranches of Trigeminal nerve
The cause of Trigeminal neuralgia • Idiopatic neuralgia - compression of the nerve’s root by upper cerebellar artery • Symptomatic neuralgia • Multiple sclerosis • Tumor of the brain stem • Cranial trauma • Inflammation diseases of nasal sinuses • Post-herpetic neuralgia • Lesion of temporal-mandible joint
Pain attack Triggerzones Painful paraspasm Clinical features of Trigeminal neuralgia
Facial nerve • Facial asymmetry • patient can’t wrinkle the forehead, close eyes, purse the lips, retract the buccal angles in a smile • impairment of taste on the anterior two third of the tongue • Bell’s symptom • corneal reflex is decreased or absent
Signs of lesion of Facial nerve before the n. Petrosus major • Paresis of mimic muscles • Dryness of eye, loss of lacrimation (xerophtalmia) • Hyperacusis • Loss of taste over anterior 2/3 of tongue • Dryness of oral cavity (xerostomia)
Signs of lesion of Facial nerve before the n. Stapedius • Paresis of mimic muscles • Lacrimation • Hyperacusis • Loss of taste over anterior 2/3 of tongue • Dryness of oral cavity (xerostomia)
Signs of lesion of Geniculate ganglion (Ramsay-Hunt syndrome) Herpetic involvement of Geniculate ganglion • Paresis of mimic muscles • Lacrimation • Hyperacusis • Loss of taste over anterior 2/3 of tongue • Dryness of oral cavity (xerostomia) • Herpes vesicular eruption in the throat or over the pinna
Paresis of mimic muscles Tears Loss of taste over anterior 2/3 of tongue Dryness of oral cavity (xerostomia) Signs of lesion of Facial nerve before the n. Chorda tympani
Paresis of mimic muscles Lacrimation Signs of lesion of Facial nerve after the n. Chorda tympani
Facial nerve Clinical examination • observation of the patient while he talks and smiles. • The patient is asked to show his teeth by retracting the buccal angles, • to whistle • to pyres the lips against the pressure of the examiner’s fingers. • slight unilateral weakness may be detected by asking the patient to blow the cheeks out fully.
Facial nerve Clinical examination • the platisma function - the patient makes a maximal effort to draw the lower lip and angle of the mouth downward and outward, at the same time tensing the skin over the anterior surface of the neck. • Taste is examined with the use of sugar, tartaric acid, sodium chloride, quinine, or similar substances. The patient is instructed to protrude the tongue; a small quantity of the test substance is gently rubbed on one side of the tongue and the patient signals identification of the test substance before drawing the tongue into the mouth to prevent diffusion of the taste to the opposite side or to the posterior third of the tongue, thus obscuring the test.
n. Glossopharyngeus n. Vagus • the voice is hoarse or brassy • dysphagia and regurgitation of fluids through the nose • the testing of taste sensation on the posterior one third of the tongue • ipsilateral paralysis of the palatal, pharyngeal, and laryngeal muscles • bilateral lesion (dyspnea, apnea, periodic respiration - Cheyne-Stokes breathing)
Function of n. Glossopharyngeus • motor • sensory • autonomic
Motor function of n. Glossopharyngeus Motor nucleus (n. ambiguus, common withX Cranial nerve) is located in medial part of oblong brain. Fibers from this nuclei are going on the back of olive, аfter that — through the jugular fosse of scull and innervate m. Stilopharyngeus
General sensation - g. jugularae superius a) Dendrites innervated posterior 1/3 of the tongue, palatine muscles, pharyngs, oticmembrane, otic cavity b) Axons are finished in nucleusalae сіnеrеа Sensory function of n. Glossopharyngeus
Taste sensation - inferiorJugularganglion a) Dendritis are going to the posterior 1/3 of the tongue b) Axons arefinished in nucleustractus solitarii Sensory function of n. Glossopharyngeus
Autonomic function of n. Glossopharyngeus • Secretion autonomic fibersstart from nucleussalivatorius, which is located in lower part of the oblong brain, preganglion firbers are going to the Otic ganglion, postganglion firbersinnervate Parotidgland
The cause of Glossopharyngealneuralgia • Compression due to the hypertrophy of processus stiloideus • Compression due to the ossification of ligament stilopalatinum • Compression due to the posterior lower cerebellar artery • Cancer on base of the tongue, tumors of the larynx
Clinical features of Glossopharyngeal neuralgia • Paroxysmal pain in tongue radix, pharynx, tonsils, lateral part of the neck, angle of the mandible • Trigger zones (tonsils, base of the tongue)
Bulbar syndrome • dysarthria • dysphagia • dysphonia • gag reflex is absent or decreased • the tongue is atrophic • paralysis is unilateral or bilateral • can be (dyspnea, apnea, periodic Cheyne-Stokes respiration)
Pseudobulbar syndrome • dysarthria • dysphagia • dysphonia • the pathologic oral reflexes are present • Involuntary crying, smiling • paralysis is only bilateral