Download
1 / 53
530 likes | 701 Views
Procedures. Basic Format Cesarean Section. Objectives. Assess the anatomy, physiology, and pathophysiology of the Cesarean Section. Analyze the diagnostic and surgical interventions for a patient undergoing a Cesarean Section.

E N D
Procedures Basic Format Cesarean Section
Objectives • Assess the anatomy, physiology, and pathophysiology of the Cesarean Section. • Analyze the diagnostic and surgical interventions for a patient undergoing a Cesarean Section. • Plan the intraoperative course for a patient undergoing Cesarean Section. • Assemble supplies, equipment, and instrumentation needed for the procedure.
Objectives • Choose the appropriate patient position • Identify the incision used for the procedure • Analyze the procedural steps for Cesarean Section. • Describe the care of the specimen • Discuss the postoperative considerations for a patient undergoing Cesarean Section .
Terms and Definitions • Obstetrics • See Indications • Same as for L & D Terms STST p. 486
Definition/Purpose of Procedure • Surgical delivery of an infant through the abdominal and uterine wall. Often performed as an emergency for abruptio placentae, placenta previa, or cephalopelvic disproportion. May be scheduled for “previous c-section.” • Performed when safe vaginal delivery is questionable or immediate delivery is crucial because the well-being of the mother or fetus is threatened
Indications • Abnormal presentations (breech, transverse, etc.) • Abruptio Placenta • Carcinoma of the Cervix • Cephalopelvic Disporportion (CPD) • Cervix will not dilate • Fetal distress** Most common reason • Habitual death of the fetus during the course of labor • Placenta Previa • Preeclamptic toxemia in pts where difficult labor is anticipated • Presence of STDs such as genital herpes • Previous cesarean section • Prolapse of the umbilical cord
Relevant A & P • Physiology of pregnancy • Female anatomy (covered last week)
Pathophysiology • Dependent on type of Indication
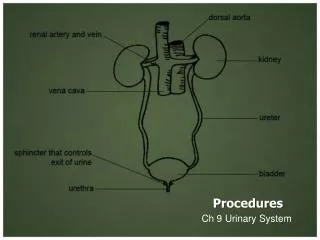
Female Pelvis: True Pelvis Inlet, Cavity (midpelvis), and Outlet
Diagnostics • Exams • Multiple methods depending on problem • Standard Assessments: Client history, determining gestational age (EDB); uterine assessment, fetal development, pelvic adequacy • Preoperative Testing: typical for any surgery (CBC, blood chemistries, U/A)
Surgical Intervention:Special Considerations • Patient Factors • Psychological status • Significant other present or not • Room Set-up: all preparations are made before the anesthetic is administered. If regional anesthesia is planned, the set-up, counts, and preliminary routines can be performed simultaneously w/anesthesia procedures. If general, the set-up, prep, catheterization, gowning & gloving of all personnel and draping are performed before anesthesia induction. Why?
Surgical Intervention: Anesthesia • Method: Regional (Epidural preferred or Spinal) or Local or General • Equipment: spinal or epidural tray • Other meds: Oxytocin (Pitocin) 10-20 u per liter of IV fluids once infant is delivered to minimize blood loss • Oxytocin may be used to induce or continue labor, contract the uterus post delivery; stimulate lactation • Carbopost (Hemabate) parenteral oxytocic used to control uterine hemorrhage following childbirth • Ergonovine, Methylergononvine (Ergotrate, Methergine) causes uterine muscle contraction
Surgical Intervention: Positioning • Position during procedure • Supine with roll at Rt hip to displace the uterus & prevent aortocaval compression • Supplies and equipment: rolled sheet for hip roll, safety belt • Special considerations: high risk areas: bony prominences; assistance PRN –awkward and in pain/between contractions
Surgical Intervention: Skin Prep • Method of hair removal: wet prep or clippers • Anatomic perimeters: Similar to laparotomy—table side to table side; to xiphoid process extending down to mid thigh: NO Vaginal prep • Solution options: Betadine or Duraprep or Hibiclens • Insert foley before prep
Surgical Intervention: Draping/Incision • Types of drapes: C-Section pack includes laparotomy drape, which may sticky clear plastic around fenestration and fluid-catching channels • Order of draping: 4 towels, abd drape • Special considerations • State/Describe incision • Skin: Low transverse Pfannenstiel (Most common) or low midline vertical; length depends on estimated size of fetus • Uterus: type depends on the need for the c-section
Uterine Incisions Kerr Incision vs Sellheim Incision vs Classical
Surgical Intervention: Supplies • General: prep set, C-Section pack, basin set, gloves • Specific • Bulb syringe for infant suction • Cord clamps, 2 per infant • Delee suction device • Cord blood tubes (2) • Blood gas tubes on standby • Suture/dressings of choice • Medications on field (name & purpose) • Catheters & Drains: Foley catheter is placed preoperatively
Surgical Intervention: Instruments • General: those for a major GYN laparotomy plus (below) or C-Section tray (facility specific) • Specific • Delivery forceps (in room), a cord clamp, mucus aspiration bulb, possible Delee suction trap, Lister bandage scissors, Foerster ring forceps, Pennington forceps, Delee retractor, (2) lab tubes for cord blood
Surgical Intervention: Equipment • General: ESU, Suction • Specific: • Infant radiant warmer mobile unit and possibly additional transport device depending on location of procedure (OR vs L & D) • Fetal monitor
Procedure Overview • The pelvis & uterus are entered. • The head of the infant is delivered & the infant’s airways are cleared • The infant’s body is delivered • The placenta is removed • The uterus is closed. • The abdomen is closed.
Surgical Intervention: Procedure Steps • Incision is made (#10 blade) and tissues of abdomen are divided w/usual fashion: have goulet or army-navy ready for muscle separation at midline & fascial incision and dissection • Peritoneal covering over bladder is palpated (to ensure no inclusion of bladder, bowel, or omentum) and incised (exposing distended uterus). 2 crile hemostats are used to elevate the peritoneum about 2 cm apart. • Bleeding sites will be clamped but not ligated until later (typically) • The uterus is quickly palpated to determine fetal placement & position • STSR: Be ready with dry lap sponges, bulb syringe, and suction
Step 7: Bladder flap retracted & transverse incision made in lower uterine segment
Surgical Intervention: Procedure Steps • Amniotic fluid is quickly evacuated from field • Assistant retracts the bladder downward with the bladder blade or other similar retractor • Surgeon nicks the uterus w/deep knife and extends the incision w/bandage scissors (blunt tips prevent injury to fetus) • STSR may be asked to remove bladder retractor & simultaneously assistant pushes firmly on upper abd while surgeon grasps infant’s head & rotates upward • Head is delivered from wound & airways immediately suctioned with bulb (poss Delee)
Surgical Intervention: Procedure Steps • STSR: Once the head is controlled, all sharp and metal objects are removed prior to elevating the infant’s head • The umbilical cord is clamped and cut. Cord blood sample is collected (surgeon may milk the cord) • The infant is passed off to the pediatrician and into the warmed crib for assessment and possible emergency resuscitation measures • STSR: Protect your sterile field • The placenta is delivered, inspected, & removed to back table (usually in a basin)
Surgical Intervention: Procedure Steps • The uterine interior may be cleaned w/a moist lap sponge. Oxytocin MAY be injected into the uterus to help with hemostasis • The surgeon closes the uterus in 2 layers with 2-0 or 0 absorbable suture (chromic catgut, Vicryl, or Dexon)—running stitch
Surgical Intervention: Procedure Steps • The bladder flap may be approximated or not—if so, a 2-0 or 3-0 absorbable suture w/fine taper needle is often used • The abdominal cavity is examined for bleeding, sponges, etc and is irrigated. • Surgeon closes abd wall and skin for low transverse incision; subcuticular stitch or staples are used for closure. • Blood clots are expressed from the uterus (STSR may be asked for basin at perineum). • Wound and vaginal area are cleaned • Dressing & perineal pad applied
Counts • Initial: Before case begins: sponges, sharps, instruments, bovie tip cleaner • First closing: Closure of uterus • Second count: beginning closure of abd cavity • Final closing • Sponges • Sharps & sm items • Instruments
Dressing, Casting, Immobilizers, Etc. • Types & sizes • Abdominal dressing and perineal pad • Type of tape or method of securing • Silk, paper, foam tape. Elastoplast for compression dressing as ordered.
Specimen & Care • Identified as: Placenta is sent per surgeon request for evaluation • Cord blood tubes x 2 filled • Blood gasses of cord may be ordered and drawn by circulator or peds from the artery within the umbilical cord • Handled: Placenta is usually sent in formalin, if sent
Postoperative Care • Destination • Allow for bonding time with infant if possible • PACU • Expected prognosis (Good, Depends on Indication and any anesthetic complications) * mortality is 4-6 times that assoc w/vaginal delivery • Maternal: healing & care of surgical wound increased risk of future C-section Infant: prognosis depends on reason for C-section and extent of oxygen deprivation
Postoperative Care • Potential complications • Hemorrhage: Fundus must be massaged just after delivery and become firm to help stop bleeding • Infection • Other: Injury to surrounding structures • Surgical wound classification: II
References • Alexander Ch 14, pp. 513-517 • www.Allrefer.com • Berry & Kohn Ch 34, pp. 694-697 • Fuller pp. 362-363 • MAVCC Unit 5
Vaginal Delivery Procedure 15-1
Labor & Delivery Terminology • Stage one: onset of labor • Stage two: complete dilatation of cervix • Stage three: birth of the infant • Stage four: after placenta is delivered