Download

1 / 27
270 likes | 502 Views
Summary results of the ERS COPD Audit programme against GOLD standards. Professor Mike Roberts (UK) and Professor Jose Luis Lopez-Campos (Spain) . Daily list of admitted patients Is COPD exacerbation the cause of admission?. No. Yes. Provisional inclusion: Candidate case. Discharge report

E N D
Summary results of the ERS COPD Audit programme against GOLD standards Professor Mike Roberts (UK) and Professor Jose Luis Lopez-Campos (Spain)
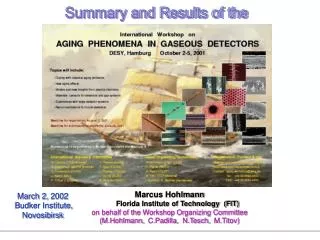
Daily list of admitted patients Is COPD exacerbation the cause of admission? No Yes Provisional inclusion: Candidate case Discharge report COPD exacerbation? No Excluded Yes Definite inclusion: Record clinical variables 90-day follow-up: Record outcomes
Hospital resources & organisation database: 48 variables – 42 variables with structure information 425 out of 432 centres that participated (98.3%) Clinical database: 127 variables – 117 variables with clinical information 16,018 cases out of 19,150 initially considered (83.6%)
Ward: Clinical area in which patients are nursed in beds as admissions to hospital. • Respiratory Department: An integrated clinical grouping of healthcare workers (clinicians and administrators) whose responsibility is to care for patients with respiratory conditions. This excludes healthcare workers whose responsibilities are purely research without a clinical role. A department may function within one hospital or across more than one hospital. • Hospital: A healthcare facility located in a particular geographical site. It may compose of one or several buildings but these buildings are administered by a single executive board. • Unit: A functional health care facility that is often identical to a hospital but may include more than one hospital and or more than one geographical location. The unit however functions as a single administrative and healthcare facility. Examples may include two, or even more, hospitals that previously were independent but have then merged clinical and administrative functions.
Characteristics of the participant hospitals in the European COPD audit Data expressed as mean (inter-country range). *P value calculated by chi-square test or ANOVA as appropriate
Resources of the participant units in the European COPD audit Data expressed as mean (inter-country range). *P value calculated by chi-square test or ANOVA as appropriate
Staffing of the respiratory units Data expressed as mean (inter-country range). *P value calculated by chi-square test or ANOVA as appropriate
For patients that require hospitalization, measurement of arterial blood gases is important to assess the severity of an exacerbation 82.4% of cases had an ABG
Oxygen therapy is the cornerstone of hospital treatment of COPD exacerbations. 13.9% of those not receiving oxygen of any kind had an admission PaO2 <8kpa 84.9% patients received controlled oxygen 9.7% high flow oxygen
Antibiotics should be given to: a) patients with the following three cardinal symptoms: increased dyspnea, increased sputum volume, and increased sputum purulence, b) Patients with two of the cardinal symptoms, if increased purulence of sputum is one of the two symptoms, c) patients that requires mechanical ventilation (invasive or noninvasive). But 79.7% patients who didn’t meet these criteria also received antibiotics 90.5% meeting these criteria received antibiotics
% Cases Antibiotics correctly prescribed by Hospitals (Austria)
Indications for Non Invasive Ventilation (NIV) include moderate to severe acidosis (pH <7.35) and hypercapnia (PaCO2>6.0kPa) without contraindications. 28.6% of patients who received NIV did not meet these criteria 51% cases with these ABG received NIV
Organisational performance of the respiratory units Data expressed as mean (inter-country range). *P value calculated by chi-square test or ANOVA as appropriate
Organisational performance of the respiratory units Data expressed as mean (inter-country range). *P value calculated by chi-square test or ANOVA as appropriate
GOLD 2010 statements according to hospital size Data expressed as mean (inter-country range). *P value calculated by chi-square test or ANOVA as appropriate
The reasons for apparent non compliance are not available to us • In some cases there may be good reason to deviate from the recommended management • In other cases this will represent poor medical practice
The variation between countries is substantial but the variation between hospitals within a single country is large too • It is likely that quality of care delivered to patients is unacceptably variable • Size of hospital and resources do not account for all the variability • We all have a responsibility to consider how to improve care across all units